Though heart is known primarily as a pump, it is the four cardiac valves that ensures the critical , non-stop unidirectional flow that sustain the circulation . It is to be recalled these valves originate in the very early days of cardiac development when the primitive heart tube loops , even as the chambers expand from primitive ventricle. Mesenchymal differentiation controlled by various genes that cleaves the valve from myocardial tissue.
While heart by itself is the supreme vascular organ , its surprising few structures inside the heart , like the valves are quiet avascular ( or is it really so ?)

The valves that beat average of 30 billion time in life time ,seem to get its nourishment from Nowhere ?
Layers of heart valve

Image source : Huk D., Lincoln J. (2017) Oxidative Stress in Cardiac Valve Development. In: Rodriguez-Porcel M., Chade A., Miller J. (eds) Studies on Atherosclerosis. Oxidative Stress in Applied Basic Research and Clinical Practice. Humana Press, Boston, MA
It’s primarily made up of complex stratified connective tissue covered by endothelial cells with intervening interstitial cells. The extracellular matrix (ECM) layers are rich in elastin proteoglycan (spongiosa) and collagen (fibrosa). It has been found myocytes and dormant fibroblasts are scattered in the valve leaflets. This forms the basis of focal origins of Cuspal Ventricular tachycardia J Cardiovasc Electrophysiol. 2002 Jun;13(6):551-6. from electricaly activated myocytes.
Is there a dynamic cell turnover within the valve tissue ? Where does it get the nourishment ? What is the effect of aging and CAD on valve tissue ?
There is growing evidence for valvular extra cellular matrix are indeed dynamic. This explains valvular lesions in connective tissue disorders like Rheumatoid arthritis. Progressive degenerative changes of aging involves remodelling , tissue engineering . Calcification of cardiac valves in endocrine disorders like hyperparathyroid states implies cardiac valvular interstitium is in continuum of systemic metabolic pool. There has been very little published evidence correlating CAD and Ischemic degeneration of valve.
Evidence for vascularity of valves
It is surprising , this simple question of vascular supply to cardiac valves has confronted the scientists for too long.
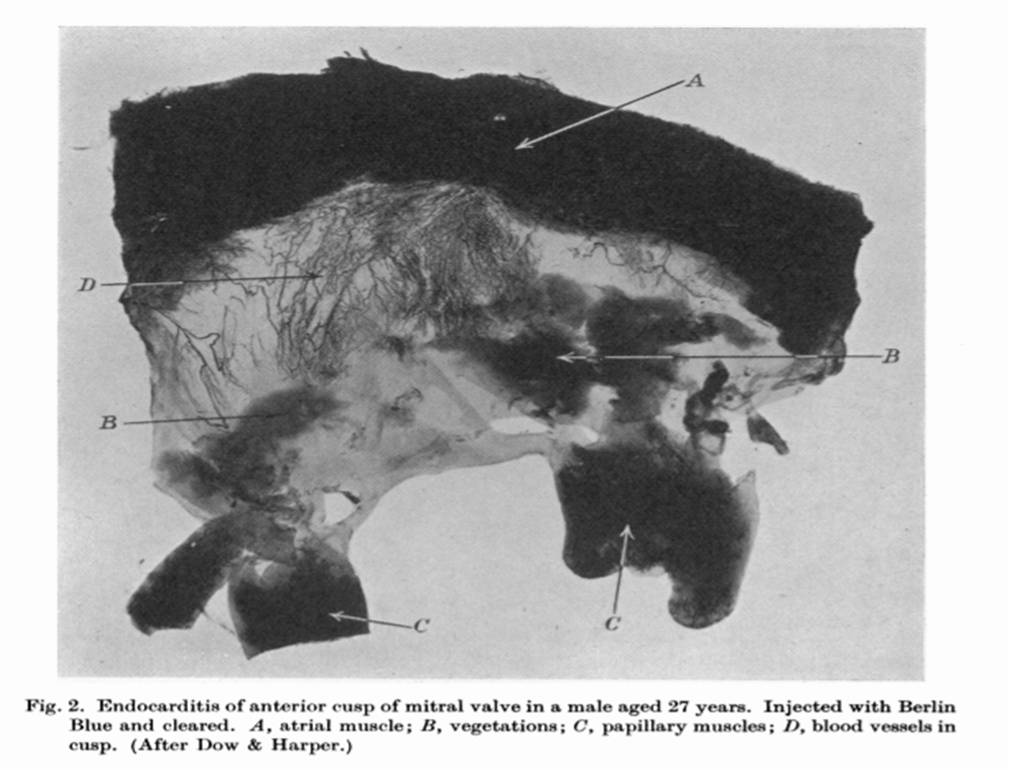
1.Histopathological and autopsy studies have revealed vascular channels.(Harper 1938 BMJ)
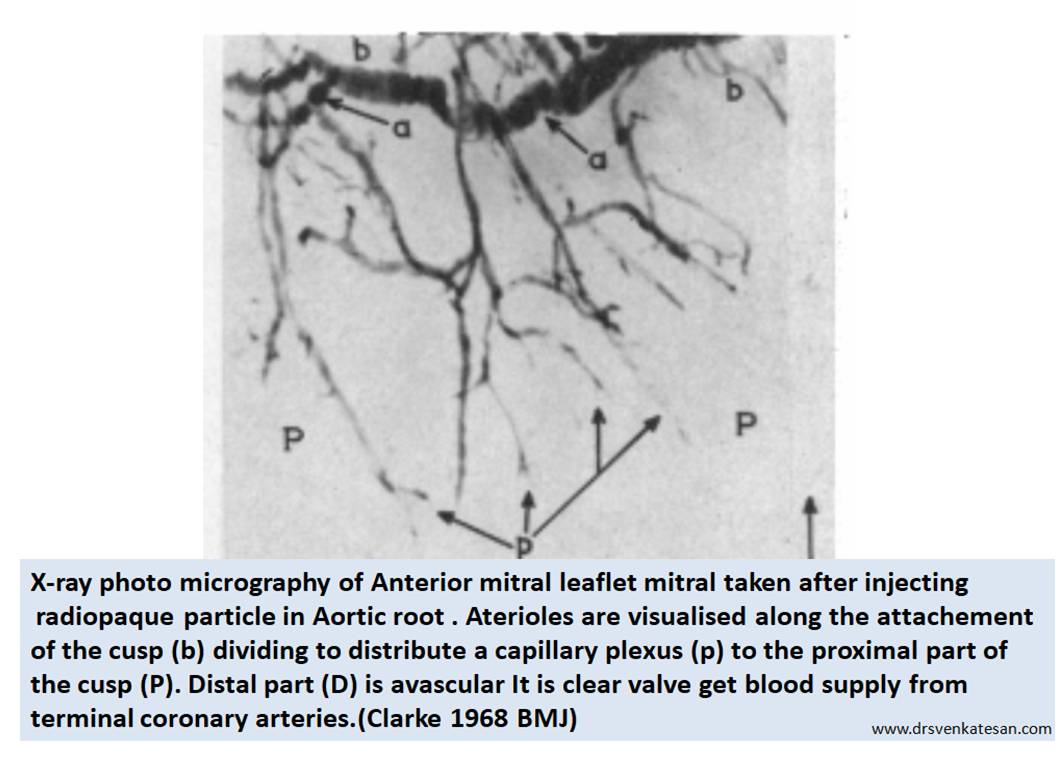
2.X-ray projection microscopy was used to image the valves after injecting radio opaque microparticles in the ascending aorta. This is probably the one of the few original studies done in UK in 1968 (Clarke et al ) it revealed significant vascularity of the valve .It was found 16 % the tricuspid valve, in 10% of the mitral valve, and was maximum in Aortic valve (24%).
3.The fact that statins reach the Aortic valve tissue in lipomatous Aortic stenosis indicate significant vascular port of entry to valves.
Direct evidence : Why don’t we ask the surgeon ?
When I asked my surgical colleagues Does the valve bleed as they cut it ? Most of them were amused with my query , still Iam not sure I got the answer right. At least one of them said since the heart is on pump , it won’t bleed any way !

Conclusive evidence : From a 1968 study
It is academically humiliating to note we have to go back 50 years in time to get a proof for vascularity in cardiac valve.(Or anything new I am missing ? readers may share !) I think , this is strongest proof for valve cusps are supplied by end coronary arteries. However the penetrance is not deep into all layers of the valve and distally

Is hematogenous spread of Infective endocarditis(IE) occur ?
How does systemic infection reach the valves ? We still believe the IE is due to direct colonisation from circulating blood .Hematogenous spread of IE do occur but difficult to prove. It seems infection of valves primarily happen from outside initiated by endothelial injury over the valves .
*There seems to be a contribution from systemic bacteremia reaching from within through the pre-existing capillary twigs as well.(Evidence elusive !)

Final message
Is cardiac valves vascular ? It is curious even in this era , we struggle to answer this query with certainity.
Yes, they are vascular structures , but at best it has partial vascular capillary network. It is also possible the valves can live a durable life even without these vascular Innervation.(I haven’t heard of a condition called mitral valve infarct or necrosis in RCA/LCX STEMI which supply the base of the heart)
Still, this partial vasculaity can become Important at times of pathology like infection or degeneration. Expecting more research in this unique area of valvular heart disease
Reference
1.JOHN A. CLARKE AN X-RAY MICROSCOPIC STUDY OF THE BLOOD SUPPLY TO
THE VALVES OF THE HUMAN HEART BY From the Department of Anatomy, University of Glasgow, Glasgow Brit. Heart J., 1965, 27, 420
2.https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC1252531&blobtype=pdf
3.Dow, D.R. and Harper, W.F. The vascularity of the valves of the human heart. J Anat. 1932; 66: 610–617
4.Ritter, S.A., Gross, L., and Kugel, M.A. Blood vessels in the valves of normal human hearts: from a study of 700 human hearts. Am Heart J. 1928; 3: 433–446
5. Saini N, Saikia UN, Sahni D, Singh RS. Vascularity of human atrioventricular valves: a myth or fact? J Thorac Cardiovasc Surg. 2014 Jan;147(1):517-21.
Read Full Post »