Bernoulli equation is the most critical equation on which the foundation of clinical Doppler echocardiography is built. Bernoulli equation tells about fluid mechanics. Bernoulli’s principle states that the sum of potential and kinetic energy of fluid per unit volume flowing through a tube is constant.
A more detailed explanation regarding Bernoulli equation is linked in this video
Applying Bernoulli in Echocardiography
So, if we can somehow measure the velocity gained across a point inside the heart we can deduce the pressure gradient. Here comes the Doppler principle that helps us calculate the velocity. Doppler is based on the reflection of sound and the Doppler shift. With the Doppler shift, we can arrive difference in velocity across a valve, or conduit. When fluid flows across a narrowed orifice (Valve /Outflow) it accelerates and builds up velocity. This gain in velocity is equal to the pressure lost ie as given by the Bernoulli equation. Since potential energy is related to height and gravity same intracardiac zones it cancels out on either side. Hence, essentially the Bernoulli pressure gradient is equal to the difference between the kinetic energy on either side.
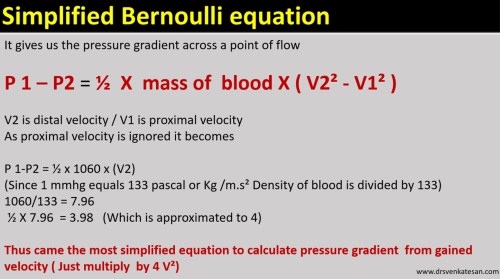
Let us see how this 1/2 of mass becomes 4. We have to convert density of blood which is 1.060 to mass.
Note : Mass = ρV . Density is mass per unit volume. So the “m” in the equation is some times referred to synonymously with the density of blood.
Application in clinical echocardiography
There has been pioneering work from Holen, Hatle and Angleson who proved the value of this equation in the clinical situation in the late 1970s. Of course, Gorlin and Gorlin worked on this similar concept in the cath lab derived pressure gradients
Reference
1.Gorlin R, Gorlin SJ. The hydraulic formula for calculation of the area of the stenotic mitral valve, other cardiac valves, and circulatory shunts. I. Am Heart J 1951:41:1-29.
2.Holen J, Aaslfd R, Landmark K, Sknonsen S, Ostrem 1. Determination of effective orifice area in mitral stenosis from noninvasive ultrasound Doppler data and mitral flow rate. Acta Med Stand 1977;201:83-88.
3.Hatle L. Noninvasive assessment and differentiation of left ventricular outflow obstruction with Doppler ultrasound. Circulation 1981;84:381-
4.Hatle L. Brubakk A. Tromsdal A. Angelsen B. Noninvasive assessment of pressure drop p in. mitral stenosis by Doppler ultrasound. Br Heart J 1978:40:131-140.