As we enter, another customary happy “New year” , a lingering “Old wish” remains largely unfulfilled. Let us try to return, to our forgotten home space, called patient’s bed side . Shall get Immersed in history taking , Intuitive clinical examination, and master the art of listening to our patient’s heart with our own ears. Investigations can wait unless it is a dire emergency.
Too often today, we bypass these foundations, relying blindly on Images, echocardiograms, angiograms, a deluge of scans, , multi-modality algorithms ,AI predictions. We have also become greedy servants to technology commerce , and increasingly intoxicating science as well. Let us not insist on investigations , driven by peer pressures or pride, in the process losing common sense in a flood of data.
Let us reclaim the intellect, that taught us listening and understanding to the patients symptoms (with kindness) is the highest form of Investigation .
Coming to scientific research, grow courage to question, debate , that ultimately would simplify complex problems .
Finally, seek the truth, which often hides behind the distorted evidence base and obsessive compulsive protocols.
While patient rights has been extensively discussed and debated , there is some concern especially in country like India, where violence against medical professionals has increased to prohibitive levels. This is mainly attributed to low levels of tolerance and high expectations from the doctors and hospitals.
There has been multiple Incidents where doctors are attacked, even when a life is lost due an incurable disease in spite of well administered treatment . Many patients are unable to differentiate the natural history of illness , any death is looked upon as medical negligence. In this context, there is a call for patient education and teaching them responsibilities and make them understand the complexity and uncertainty in the science of biology, and also accept the reality of inadvertent errors in judgment and execution in medical practice.
A curious solution is suggested .Yes , its called Hippocratic Oath : Patient version .The father of medicine would have never thought , a day would come , when patients might, try to prevail over the Doctors .Readers may decide about the political correctness , utility and practicality of such an oath.
Greetings from Chennai. It all started with some flashy classroom scribblings in Madras Medical College in the year 2008. I never imagined it would reach nearly two decades of writing. It has since reached 6 million visits in 180 countries. My thanks to all those readers and followers for making this possible. As per the request of many of you, it’s been converted to eBook format on Amazon Kindle. It is arranged in a yearly fashion .Currently published as Volume 1 . It will be live document and continuously updated.
Each and every article of the past and the future will continue to be open source on this site. Again, I shall reiterate , the book format is published only to facilitate learning in a single book format and with near- zero commercial Intent. If I do, it will be against the core concept and ethics of this academic endeavor. Of course, whatever little readers think they can contribute by buying this E-book, it will help sustain this site. Sharing the link to the book. I think as of now it is live only in India. Soon it will be globally available. https://amzn.in/d/euhL5vu
What is the purpose for us , being the part of this world ?
Why time , space, mind are almost one and the same ?
Spend few minutes here in this video. Not every one is blessed to reach the space station .But thanks for this effort by Sen , we can see the astronauts eye view of our lovely planet . Do you see any unrest ? How many of you are seeing 5 million life forms here, other than human beings ?
As cardiologists , we are struggling round the clock ,to salvage even few milligrams of myocardial damage. Meanwhile, how could the world be a mute spectator, to all those fights for silly things in life , and allow, war, violence, poverty, greed & commerce, take more lives than diseases ? It is very very clear , doctor’s role in alleviating human suffering is far less than, what we Imagine.
This book is dedicated to all those amazing scientists of the past & present who laid the foundation of modern medicine with their selfless hard work. Footprints of their legacy can be felt in everything we do in our daily clinical practice.
Hope, at least few of the readers get inspired by this book. It is available in both print and kindle versions. Let me state, with all honesty, this book is written with zero commercial interest. ( I guess , publishers somehow read my mind .The agreement clearly says the author can get only about 25 % the sale value of a book. That’s fine. May be it will help running this website.
Surprised to find the book in this month’s best seller in Medical history category . I don’t know how is this possible ? as the total number copies sold are still less than 100, since published !
Now, you can view who all are reading this site live on a revolving globe. It makes all the more happier to note that all these grateful and honourable dots (i.e., you) are literally drawing the world map . Six million reads from 190 countries, right from the Solomon Islands in Micronesian Pacific, abutting the International date line, to the extreme west, reaching Chile and Hawaii has happened so far.
This is a 15-year-old post about LVH, written in 2008. Few of my colleagues, now agree with this, but still hesitate to oblige in the open, suggesting it is too good to be true! Re-posting it for your own assessment. Surprised, why cardiology community didn’t consider this observation worthy to pursue.
Advantages of Left ventricular hypertrophy (LVH)
Left ventricular hypertrophy is one of the most common clinical cardiac entity.It is recognised either by ECG or echocardiography.LVH has a unique place in cardiology as it can imply a grossly pathological state or a marker of healthy heart as in physiological hypertrophy in athletes.
Logic would suggest, in this era of stem cells and nano medicine , every muscle fibre in ventricle is worth in gold !. So when the nature provides an extra reserve of myocardium in the form of LVH one should welcome it, if otherwise not harmful.
Is LVH due to systemic hypertension benign ?
Not really, LVH has been shown to be an independent cardiac risk factor. (The famous Framingham study)Further LVH can result in diastolic dysfunction and the risk of cardiac failure increases.
But in spite of these observations, an astute clinician with considerable experience will appreciate , patients with LVH fare better during an acute coronary syndrome !
This has been a consistent clinical observation . (Shall we call it as class C . ACC /AHA evidence? )
Is LVH an asset during ACS ?
A hypertrophied heart takes ischemic injury very easy , it doesn’t really hurt much . Another possibility is that in LVH myocytes are relatively resistant to hypoxia .
Patients with LVH rarely show significant wall motion defect following an STEMI.This is probably because the full thickness transmural necrosis is almost never possible even if extensive MI occurs.
This is also reflected in ECG as these patients rarely develop q waves in following STEMI .
Persistent ST elevation and failed thrombolysis is very uncommon in pateints with LVH.
LVH provides a relative immunity against development of cardiogenic shock . It requires 40% of LV mass destruction to produce cardiogenic shock.This can rarely happen in LVH. In a long term analysis we have found none of the patient with LVH developed cardiogenic shock following STEMI.
LVH patients are also protected against development of free wall rupture.
Concluding message
“Lack of published evidence is the weakest evidence to dismiss a true myth”LVH , either pathological or physiological, has a hitherto unreported beneficial effect.It acts as a myocardial reserve and helps limit the impact of STEMI.
Pardon ,this video is nothing to do with cardiology. It is from the archives of the United nations library .This can teach some important lessons in art of communication , sharing to all folks, especially medical students. It was recorded in 1959 in Newyork, UN head quarters.Four 17 year old school girls & boys were invited for a debate on a complex topic. Does God exist ? How do you pray ? and what is the purpose of different religions ?
I keep wondering , how these youngsters accumulated so much wisdom and express it in such a polite manner too. Mind you, this was recorded , when learning happened with out any digital aids.The word Internet was unheard off. No ego, no bluntness, no diatirbes that has become a norm in many debates now. I got a punching lesson from this clip, be gentle when taking extreme views in any topic.
I wish, every medical debate in class rooms should happen this way.The key to succesful debate is, to accumulate knowedge, willingness to question the convention, and respecting the oppositie point of view.
The high point of talk show, was, when the Brazilian girl(due respects, she should be nearing 80 years now) tell us casually some things are not meant to be understood in life .I tell the same when some patients ask too many questions about their illness which may not have an answer.
Wishing every one of you an Enlightening New year. As we begin a new journey around the sun, yet another time, let us re-dedicate ourself, to use science, for the welfare of our planet & people.
Thank you , for visiting this site and make all its worth.
Just one memory of 2022, lingers ! Retired and left Madras medical college,Chennai after 3 decades, which grew me up as a Cardiologist.
“I thought, he was not the right patient for the procedure. I believe, what I did was the correct decision. Why all this fuzz? after all, the patient is doing so well without that procedure,.. are you worried about that?
“No, I need an explanation, we have a fully functional cath lab in our center. The patient came in the right window period. Still, you haven’t offered the best mode of treatment”.
“I can reiterate it again sir. Just because a lab is available 24/7, it doesn’t make all patients eligible for a PCI. I think I didn’t commit a professional misdemeanor when I decided in favor of fibrinolysis. In fact, I would be guilty had I rushed him to the cath lab, just to satisfy the misplaced scientific position we have decided to adopt. If you think, I am culpable for successfully treating a patient without taking the patient to the cath lab, you may proceed with the penal action.
Before that, I would request you to please read the current edition of this book we all revere. (Which continues to mentor physicians all over the globe for the past 50 years)
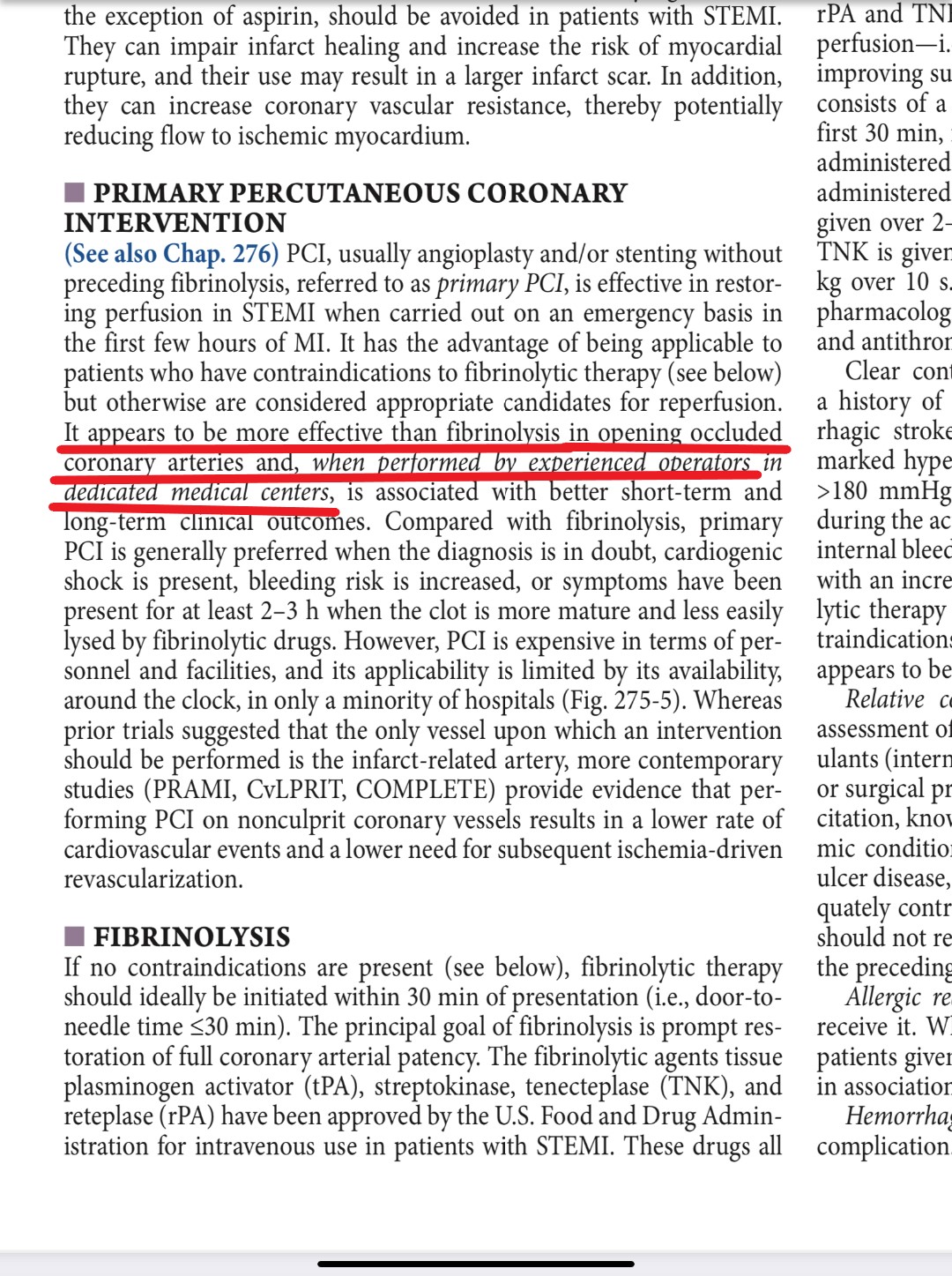
The current edition of Harrison 2022 is just out. I thought, there is something great learning point in Cardiology chapter, specifically about the reperfusion strategies in STEMI
My hearty thanks to the editors of the chapter for the crystal clear expression about this much-debated procedure* and specifically choosing the word “PCI appears* to be more effective ” (even) if it is done in experienced persons in dedicated centers. The choice of the word used by the authors is Intentional and must be applauded. This message must be propagated to all our fellow physicians. What a way to convey an important truth pertaining to the management of the most common cardiac emergency, while many in the elite specialty are so dogmatic in their assertion without verifying the reality.
* The verdict is still under the jury even after 3 decades, since the PAMI days of the early 1990s. Thank you, Harrison. What a gentle, but a righteous way to express an opinion about a procedure that is apparently enjoying a larger-than-life image based on a handful of studies and a flawed meta-analysis.
Final message
Primary PCI is just an alternateform of treatment to fibrinolysis in STEMI. Both are equipoise in the majority of patients. Extreme care and diligence are required to harvest the small benefit the PCI seems to provide. There are lots of ” if and buts” that decide the success of this procedure. Get trained, and do it selectively for those who really need it.
Postamble
You may call yourself a super-specialist. But, please realize, If you have any doubt about key management strategies, never feel shy to take a cue from Internal medicine books. The greatness of these warrior books is that, it comes devoid of all those scientific clutters backed by premature evidence.
Dr.Richard Asher, a British physician from Sussex addressed a group of young passing out medical students way back in 1948 in London. The lecture was titled seven sins of medicine! We should thank the Lancet for having published this brief speech the subsequent year in its journal making it immortal medical teaching!
Though he was listing these sins among medical students, it is very relevant to every health professional.
1.Obscurity
Asher endorses the use of clear communication and plain language whether writing or speaking. Obscurity may be used to cloak one’s own ignorance, or due to an inability to communicate with those outside of the medical profession. “If you don’t know, don’t admit it. Instead, try to confuse your listeners.” is not uncommon. Regardless of the intention, whether to misdirect from incompetence or to foster a feeling of superiority, the patient and those surrounding them are often left confused and uncertainiy.
2. Cruelty
This sin is perhaps one of the most commonly committedby doctors and medical students. Whether it be the physical thoughtlessness of a half-dozen students palpating a painful tumor mass, or loudly taking (or presenting) a patient’s history in a crowded room, one of the first things that is unlearnt by a medical professional is to treat the patient as they themselves would like to be treated.
3.Bad Manners
Often overlooked, rudeness or poor taste in humour is condoned within the hospital setting. At the end of the day, many doctors and students are simply rude to patients that do not suit them. Whether it is a snapping at an uncooperative patient or making a cruel joke about them after leaving the room, the impact of these “coping mechanisms” (as they are considered to be by many) must be taken into account.
4. Over-Specialisation
In a growing trend by the medical establishment, over-specialization and under-generalization is a growing problem in the wider medical community. Ignoring aspects of one’s education in favor of more interesting aspects is a behavior that is pathological and outright negligent in a student. Failure to diagnose or to treat a patient because “their signs and differential fall outside of my field, let’s turf them to another service” ought to be a seriously considered Supervisory & Training issue.
5.Love of the Rare
(aka “If you hear hoof-beats, think horses. Not zebras”) The desire for rare and interesting diseases causes many medical students and young doctors to seek the bizarre rather than seeing a mundane diagnosis.
6. Common Stupidity
As well as the standard definition for this sin, the specific example of “using empirical procedures rather than tailoring for the patient” or the young doctor “flying on autopilot” must be mentioned. Ordering another test that is redundant, and for which the results may already be interpreted from the history, before starting treatment is such a situation. For example: requesting a hemoglobin count before beginning transfusion, despite the fact that the patient appears obviously anaemic.
7. Sloth
Laziness. Also includes ordering excessive numbers of tests, rather than simply taking the time to take an adequate history
Final message
It is astonishing, to note Dr.Asher made this observation in the very early days in the evolution of modern medicine,(No critical care units, no HMOs, No industry nexus with research, & commodification of medicine ) I wonder what Dr. Asher would have to write if he is alive in 2021.
Wish, every medical professional shall find their Asher score. Looking back on my career, I must confess my score would be 3 ( may be 3.5 !) out of 7. Now, desperately trying to get rid of them. Mind you, the 4th (Overspecailisation) and 6 th (common stupidity) is inherently built into the system. I think, very tough to avoid them.
This 90-second video clip is a “perfect provocation”
Allan Savory is a renowned ecologist from Africa. He is a global leader in environment and eco protection. He is making this famous comment, during one of his interviews from the deep forests of Zimbabwe, after years of ground-level work in the field of desertification and climate change. I can understand his feelings, as we also encounter similar situations at ground zero of the health care delivery system.(I wonder if there is anything called peer-reviewed bedside caring)
We realize wide gaps between academia, patient care, and research are the norm, not an exception. One reason for this is, even well-learned medical professionals find it difficult to comprehend, that the practice of medicine is essentially an art, administered with love, care, service-mindedness. A cost-effective infrastructure with an immense amount of teamwork is critical ( Of course, guided by a fair amount of knowledge, expertise based on good scientific principles)
Final message
As Savory says, let us hope, the future looks bright, that welcomes young researchers from the fringes of the scientific community. Let them be conferred with all courage and resources to course-correct medical science from its frequent aberrant and awkward turns.
I haven’t clearly understood the true meaning of customary Dr tag, my name carries for more than 3 decades, till I saw this. Wish, this video is played to all young medical students on their graduation day.
I am realizing with guilt, it requires a Holywood movie buff to remind us the true meaning of the famous WHO – definition of Health, done in the most holistic fashion in the year 1948.
Health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.
So, technically, whoever serves to improve these three components and alleviate human suffering becomes a doctor.
Happy to share this on July 1st, the official Doctor’s day in India in memory of the Bharat Ratna Dr.B.C.Roy of Bengal.
Reference
The clip is from the movie Patch Adams, Directed by Tom Shadyac. A Hollywood celebrity movie maker, Virginian professor of communication turned philanthropist, now retired to a minimalist life. He is also known for his famous documentary I amthat talks about the problems faced by the world. Though his works are much appreciated, I must say, they are underrated. Deserves more than an Oscar for communicating his thoughts on the medical profession perfectly and for social equality.
I think it is an Invalid question. Whether you like it or not , medical science and philosophy are always bonded together and its relationship is eternal. It doesn’t make sense to separate them. I think we have misunderstood the meaning of philosophy. While science is presumed truths, philosophy is trying to believe in unknown truths. Philosophical truths are built-into every decision a medical professional takes.
If the expected natural history of any disease is science, unexpected deviations are philosophy. (RT PCR testing for diagnosing Corona is science, why 90% of them are not infective and don’t transform disease is philosophy) When something is not seen or quantifiable like human immunity, it is a perfect example of concealed science or manifest philosophy.
Taking about what we think we know is science, Talking about what we really don’t know is philosophy. The term Idiopathic syndrome finds a proud of the place in every specialty in medicine, Isn’t?
What will be your answer when your patient wants an assurance that a stent, you had just implanted will not get occluded in the next 6 months or so.“I don’t know, I cant assure you about that” will be your most likely answer. (Though, we do it in style, hiding behind the scientific hyperbole decorated with numbers, also referred to as statistics) Please realize, this is the expression of medical philosophy in the finest form.
Final message
My Impression is, philosophical truths should be liberally used in a regular fashion right from the first-year medical school to advanced specialty teaching. This seems essential as science in the current times suffers from too much sanctity. This has spilled over to the doctor population as well, and make them appear invincible.
If only we realize science often trailsbehind the philosophical truths at least by a few decades, our patients will not be injured inappropriately and prematurely. Mixing science with philosophy in the right composition ( aperfect academic cocktail ) will bring out the best from the noble profession.
Postamble
Can anyone guess, why scientists are given a doctorate in Philosophy degree (PhD ) ?
A young man aged around 40 years, had a STEMI was promptly thrombolysed in a small hospital located about 40 KM away in the suburbs of my city Chennai. They did an awesome job of saving the patient life and salvaging the myocardium.
Now begins the story . . . one of the non-medical person who is the owner of the hospital has an unfortunate working business relationship with a frighteningly big nearby hospital which had signed a memorandum of irresponsible understanding . It demanded any patient who arrives in the small hospital with MI should be transferred at earliest opportunity to them.
So, an ambulance was arranged and the patient (with a fairly well reperfused heart ) was shifted in an emergency fashion . It reached desired destination after nicely chugging along the choked chaotic Chennai evening traffic for 45 minutes.
The guy was taken directly to cath lab through the side doors to perform a second salvage procedure on a successfully opened IRA. Young cardiology consultants in designer cath suite welcomed the smiling ACS patient to their posh new lab .Did few rapid radial shots, mumbled among themselves for few minutes, decided to stent a minimal LAD lesion for a patient who was in zero distress with well-preserved LV function.
*The relatives of the patients were curious when they were asked sign a fresh set of consent which elaborately mentioned about possible life risk during the procedure.
The patient’s wife was clearly amused and she pointed out to the superior cardiologists about the earlier briefing by the Inferior freelance cardiologist who treated him in the previous hospital. She recalled , “I was told in confident terms that Initial thrombolysis has been spectacularly successful and bulk of the treatment is over and risk of complication has dramatically reduced”.
Then why is this distressing risk taking story again , she asked ?
The doctors hurriedly explained ,”this procedure is different. We are sorry to say we have no other option but to add further risk to you” ! but , its all for your good !
Why should I ? If the initial lysis is very successful why do you want to meddle with it again ?
No Madam , you are ill-informed , you can’t talk like that .This is what modern science is all about. Leave the professional decision to us. We need to check immediately whether the lysis is really successful .We can’t rely on the ECG.Further, true success lies in stenting the lesion as we fear the ill-fated site may close again.We are taught to practice protocols based on standard scientific guidelines. This hospital has highest rating in-terms of quality care. That’s why we got updated ISO 2000 NABH accreditation
The women who is a soft ware engineer was smartly and scientifically silenced in 5 minutes flat !
Post-amble :
What happened to the patient then ? (When you fear something it happens is in’t the Murphy’s law ?)
The apparently asymptotic and comfortable patient had uneventful PCI. A long drug eluting stent was implanted in recanalized lesion in LAD with around 30 % narrowing that ended with an innocuous looking diagonal pinch. The procedure was uneventful , however next day he developed some fresh ECG changes and chest pain . The worried team took him for another angio found stent was patent But , ultimately after a stressful 3 days of stay , some thing went wrong he ended up with new LV dysfunction.He got discharged fine with a caution that , his stent needs to intensively monitored for the next 1 year since technically he had recurrent ACS !
Lessons we don’t learn from such cases.
When two procedures are done to accomplish the same aim (Reperfusion) , but with differing success rates, expertise, time ,and unpredictable hazards , the benefits from them may not add together. There is clear knowledge deficit here. Scientific data can never provide fair answers to these questions as all real life cofounders can never be recreated in study population.
While we expect 1+1 to become two in pharmaco-Invasvie strategy ,one should realise it may end up with either zero or even – 2 .
1 -1 = 0
-1 + (-1)= -2 ?
Learning cardiology from lay persons
The patient’s shrewd wife threw this question ,
After two modes of re-perfusion done sequentially in my husband’s heart , at a total cost of Rs4.5Lakhs Why he is still left with significant LV dysfunction (Which was around 40% EF.)
The query raised by the lady appeared much more crucial and logical than the ones discussed in many top-notch live interventional workshops we attend every few months!
As usual , I started mulling over the issue. There is something wrong with the way , we understand the pharmaco invasive approach-PIA .You go with it only if initial pharmacological approach has failed.
Of Course ,there is one more modality possible ie Pharmaco -Angio strategywhere in, you look at the coronary anatomy and take a call ! This sounds good , the only issue is taking a right call! My experience suggests wrong calls are the rule and exceptions are rare. Then a whole new issue erupts about all those non IRA lesions
Final message
So, til we have gain complete self-control over our evolved ignorance and evolving knowledge , it is better to follow this proposed funny new ACS algorithm called “Pharmaco -non invasive” approach (PNIA) in asymptomatic ACS patients who have had apparently successful lysis.
*Please note, Incidentally PNIA actually refers to simple good old traditional stand alone thrombolysis.
Counter point
No one can deny Interventional cardiology carries a risk of untoward effects.Don’t blow this out of proportion. Do you know, how many lives have been saved by routine Pharmaco -Invasive approach ?
I am not sure , my experience may be limited.Let me ask the readers. Is routine PIA is warranted in all asymptomatic , successfully lysed STEMIs ?
100% occlusion of a coronary artery result in STEMI.This includes both thrombus and mechanical component .We are very much blinded till we touch , feel and see the lesion with a wire or IVUS to quantify the mechanical component’s contribution in the genesis of STEMI.It is generally believed (True as well ) thrombus is the chief culprit .It can even be 100 % thrombotic STEMI with just a residual endothelial erosion and hence
zero mechanical component .However , the point of contention that non flow limiting lesion is more likely to cause a thrombotic STEMI than a flow liming
lesion seems to be biased and misunderstood scientific fact .
What happens once 100 % occlusion take place ?
Sudden occlusion , is expected to evoke a strong fire fighting response within the coronary artery.The immediate reaction is the activation of tissue plasminogen system. In this aftermath few succumb . ( Re-perfusion arrhythmia generated as VF ) .The TPA system activates and tries to lyse the clot.The volume , morphology, attachment, content of thrombus , and the elasticity of fibrin mesh , location of platelet core would determine the life and dissolvablity of thrombus. Even a trickle flow can keep the distal vessel patent .(Please note a timely TIMI 2 flow can be a greater achievement than a delayed TIMI 3 flow !)
What happens to the natural history of thrombus in STEMI ?
Thrombus formed over the culprit lesion can follow any of the following course
Can remain static
Get lysed by natural or pharmacological means
Progress distally (By fragmentation or by moving en-mass )
Grow proximal and and involve more serious proximal side branch obstruction
Organise and become a CTO
Factors determining thrombus migration
The interaction between the hemodynamic forces that push a thrombus distally and hemo-rheological factors that promote fresh proximal thrombus formation are poorly understood. The altered intra-coronary milieu with a fissured plaque covered by platelet vs RBC / fibrin core, totally of obstruction, reperfusing forces , re-exposure of raw areas and the distal vessel integrity all matters.
While, logic would tell us, thrombus more often migrates distally assisted by the direction of blood flow, an opposite concept also seeks attention , ie since the blood flow is sluggish in the proximal (to obstruction site )more thrombus forms in segments proximal to obstruction.
(In fact, its presumed in any acute massive proximal LAD STEMI , it takes hardly few minutes for the thrombus to queue up proximaly and clog the bifurcation and spill over to LCX or even reach left main and result in instant mechanical death.)
What is the significance of length and longitudinal resistance of the thrombotic segment in STEMI ?
If thrombus is the culprit let us get rid of it , this concept looks nice on paper , but still we don’t know why thrombus aspiration in STEMI is not consistently useful. We also know little about the length of the thrombotic segment .When a guide wire is passed over a STEMI ATO it may cross smoothly like “cutting a slice of butter” in some , while in few we struggle and end up with severe no-reflow inspite of great efforts .Why ?
What is the Impact of distal collateral flow in flushing fresh thrombus ?
The efficacy of collateral flow in salvaging myocardium is underestimated. Distal vessel flow if perfused partially by acute collaterals the thrombus load is not only less it’s soft and fail to get organised early that would help cross the lesion easily.
Mohandas Karam Chand Gandhi , father of my country , India , made these observations in year 1925 about the fundamental constituents of violence in society . These words of monumental wisdom came when he was addressing young Indians in a country- side rally .
Note, his finger points to , what exactly is relevant to our profession ! He emphasized this nearly 100 years ago, when medical science was at its infancy .One can only guess what would be Mahatma’s comment about our profession in it’s current form !
Should we include moral, behavioral and ethical classes right from the first year of medical school along with Anatomy , physiology and bio chemistry.Medical council of India obviously need to burn more mid night oil , I wish it happens in my life time. !
I don’t know, any one has tried to differentiate the mechansims of dyspnea with reference to systolic and diastolic dysfunction .We have made some observations in certain group of patients during EST . I do not know how far one would agree with this .
For the same amount of stress or work load persons with systolic dysfunction behave differently . However ,both will complete the activity but the onset and perception of dyspnea is slightly different in patients with predominant diastolic dysfunction.
Diastolic dyspnea (Dyspnea due to predominant diastolic dysfunction / HFPEF)
Delayed dyspnea . It manifest well after the exertion is completed.
It is more off a struggle to handle the venous return .The forward flow (Arterial circuit ) is relatively well toned and tuned and hence fatigue is rare .
Typically it has a prolonged recovery time .(? > 1-2 minutes )
Is it less harmful in terms of longevity ? May be . . . since it is more related to physical de-conditioning. Most of the physiological episodes of dyspnea are probably diastolic dysfunction mediated .
Dyspnea that is triggered in diastole is also dependent very much on the heart rate .If the heart rate fail to reach the baseline the recovery of dyspnea is also delayed
Some believe , physiological dyspnea should disappear within 30-60 seconds after termination of activity .(Highly arbitrary!)
Systolic dyspnea (Dyspnea due to predominant systolic dysfunction )
Patients with primary systolic pump failure experience dyspnea very early into exercise .
Much of dyspnea occur during activity itself .
Exercising muscles show hypoxia and hence fatigue is conspicuous .
Recovery of dyspnea is relatively immediate as the activity is stopped .Demand from exercising muscle is significantly dropped.
If the venous return is well handled by the ventricles the recovery phase is more comfortable .
Summary
In primary diastolic dysfunction ,the maximum stress to ventricle occurs when the venous return peaks that usually happen in the exercising muscles , as they shed vaso-dilatory property in post exertion phase .
Management Implication
Fluid overload , Tachycardia are more related to diastolic dysfunction .(Beta blockers by prolonging the diastole can , provide important relief of dyspnea in diastolic dysfunction (In HOCM patients this action could be more important that the much hyped negative inotropism !)
Final message
Dyspnea is a complex cortical perception , influenced by filling pressure of heart, stretch receptor in lungs , respiratory and exercise muscle . It is further impacted by number of biochemical parameters (Lactate/ O2 etc )
Of-course , it could be a far fetched imagination to split dyspnea mechanism with reference to cardiac cycle. Combinations of both systolic and diastolic dysfunction is the norm in many cardiac conditions . However , I believe we need more insight in the pathogenesis of this , “most important symptom” that emanate from the heart .
Prosthetic valve implantation has revolutionized the management of valvular heart disease . The original concept valve was a ball in a cage valve , still considered as a fascinating discovery. It was conceived by the young Dr Starr and made by Engineer Edwards .This was followed by long hours of arguments, debates and experiments that ran into many months . The silent corridors of Oregon hospital Portland USA remain the only witness to their hard work and motivation. At last, it happened , the first human valve was implanted in the year 1960. Since then . . . for nearly 50 years these valves have done a seminal job for the mankind.
With the advent of disc valve and bi-leaflet valve in the later decades of 20th century , we had to say a reluctant good-bye to this valve.
There is a lingering question among many of the current generation cardiologists and surgeons why this valve became extinct ?
Starr and Edwards with their child !
We in India , are witnessing these old warrior inside the heart functioning for more than 30 years.From my institute of Madras medical college which probably has inserted more Starr Edwards valve than any other during the 1970s and 80s by Prof . Sadasivan , Solomon victor , and Vasudevan and others .
It is still a mystery why this valve lost its popularity and ultimately died a premature death.The modern hemodynamic men working from a theoretical labs thought this valve was hemodynamically inferior. These Inferior valves worked like a power horse inside the hearts the poor Indian laborers for over 30 years.
A Starr Edwards valve rocking inside the heart in mitral position
The cage which gives a radial support* mimic sub valvular apparatus, which none of the other valves can provide.
* Mitral apparatus has 5 major components. Annulus, leaflets, chordae, pap muscle, LV free wall.None of the artificial valves has all these components. Though , we would love to have all of them technically it is simply not possible. The metal cage of Starr Edwards valve partially satisfies this , as it acts as a virtual sub valvular apparatus.Even though the cage has no contact with LV free wall, the mechano hydrolic transduction of LV forces to the annulus is possible .
Further , the good hemodyanmics of this valve indicate , the cage ensures co axial blood flow across the mitral inflow throughout diastole. .Unlike the bi-leaflet valve , where the direction of blood flow is determined by the quantum of leaflet excursion in every beat . In bileaflet valves each leaflet has independent determinants of valve motion . In Starr Edwards valve the ball is the leaflet . In contrast to bi-leaflet valve , the contact area of the ball and the blood in Starr Edwards is a smooth affair and ball makes sure the LV forces are equally transmitted to it’s surface .
The superiority of bi-leaflet valves and disc valves (Over ball and cage ) were never proven convincingly in a randomized fashion . The other factor which pulled down this valve’s popularity was the supposedly high profile nature of this valve. LVOT tend to get narrowed in few undersized hearts. This can not be an excuse , as no consistent efforts were made to miniaturize this valve which is distinctly possible.
Sudden deaths from Starr Edwards valve .
Almost unheard in our population.
The major reason for the long durability of this valve is due to the lack of any metallic moving points .
Absence of hinge in this valve confers a huge mechanical advantage with no stress points.
A globe / or a ball has the universal hemodynamic advantage. This shape makes it difficult for thrombotic focus to stick and grow.
Final message
Science is considered as sacred as our religion . Patients believe in us. We believe in science. A good durable valve was dumped from this world for no good reason. If commerce is the the main issue ( as many still believe it to be ! ) history will never forgive those people who were behind the murder of this innocent device.
Cardiologists and Cardio thoracic surgeons are equally culpable for the pre- mature exit of this valve from human domain. Why didn’t they protest ? We can get some solace , if only we can impress upon the current valve manufacturers to give a fresh lease of life to this valve .
This was written originally in 2009 early days of this blog. Now, re-posting it in 2021 , wonder any one has new data on this!
We know diabetes, smoking, hyperlidemia, hypertension are major risk factors for progressive vascular disease. They damage the vascular endothelium either directly or indirectly , by aggravating the atheroscelortic process . Diabetes apart from affecting the medium sized arteries , also affect the microvasculature. Smoking has a direct effect on endothelial function .It depletes vascular nitric oxide. High levels of circulating lipids injures the sub endothelial structures and invades the media by entering macrophages .So , all these 4 risk factors either operate independently or interact with each other and result in progressive vascular disease.
While we believe , these risk factors do not have any bias in attacking the human vascular tree, in the real world it is observed they have their own behavior pattern and have unique predilection and a deadly alliance .
For example , in chronic smokers TAO is the commonest manifestation , thrombo angitis is far too less common to occur in the coronary arteries.
Similarly hypertension per se rarely results in an acute coronary syndrome while it is the single important cause for cerebro vascular disease. Diabetes especially in women has very strong predilection for CAD , while diabetic per se is a lesser risk for stroke. Hyperlipedimia may be the one which has fairly even risk throughout the vasculature. Similarly there is a difference in renal and carotid arterial involvement with reference to the conventional risk factors .
Why this apparent difference ?
We are unlikely to get an answer to this question in the near future . Left to the youngsters . . . of tomorrow !
* Note of clarification
The source for the above chart is collected from various studies and also a huge observational data from our hospital. There could be some geographical variation , a given individual may respond differently to these risk factor depending upon his genetic predisposition and susceptibility . So the above data can be applied to general population and not to a individual.
It is often said life is a cycle , time machine rolls without rest and reach the same point again and again . This is applicable for the knowledge cycle as well .
We live a life , which is infact a “fraction of a time”(<100years) when we consider the evolution of life in our planet for over 4 million years.
Man has survived and succumbed to various natural and self inflicted diseases & disasters. Currently, in this brief phase of life , CAD is the major epidemic , that confronts modern man.It determines the ultimate life expectancy . The fact that , CAD is a new age disease and it was not this rampant , in our ancestors is well known .The disease has evolved with man’s pursuit for knowledge and wealth.
A simple example of how the management of CAD over 50 years will help assess the importance of “Time in medical therapeutics”
1960s: Life style modification and Medical therapy is the standard of care in all stable chronic CAD The fact is medical and lifestyle management remained the only choice in this period as other options were not available. (Absence of choice was a blessing as we subsequently realised ! read further )
The medical world started looking for options to manage CAD.
1970s : CABG was a major innovation for limiting angina .
1980s: Plain balloon angioplasty a revolution in the management of CAD.
1990s: Stent scaffolding of the coronaries was a great add on .Stent was too dangerous for routine use was to be used only in bail out situations
Mid 1990s : Stents reduced restenosis. Stents are the greatest revolution for CAD management.Avoiding stent in a PCI is unethical , stents should be liberally used. Every PCI should be followed by stent.
Stents have potential complication so a good luminal dilatation with stent like result (SLR) was preferred so that we can avoid stent related complications.
2000s: Simple bare metal stents are not enough .It also has significant restenosis.
2002: BMS are too notorius for restenosis and may be dangerous to use
2004 : Drug eluting stents are god’s gift to mankind.It eliminates restenosis by 100% .
2006: Drug eluting stents not only eliminates restenosis it eliminates many patients suddenly by subacute stent thrombosis
2007 : The drug is not the culprit in DES it is the non bio erodable polymer that causes stent thrombosis. Polymer free DES or biodegradable stent , for temporary scaffolding of the coronary artery (Poly lactic acid ) are likely to be the standard of care .
All stents are potentially dangerous for the simple reason any metal within the coronary artery has a potential for acute occlusion.In chronic CAD it is not at all necessary to open the occluded coronary arteries , unless CAD is severely symptomatic in spite of best medical therapy.
2007: Medical management is superior to PCI in most of the situations in chronic CAD .(COURAGE study ) .Avoid PCI whenever possible.
2009 :The fundamental principle of CAD management remain unaltered. Life style modification, regular exercise , risk factor reduction, optimal doses of anti anginal drug, statins and aspirin is the time tested recipe for effective management of CAD .
So the CAD therapeutic journey found it’s true destination , where it started in 1960s.
Final message
Every new option of therapy must be tested against every past option .There are other reverse cycles in cardiology that includes the role of diuretics in SHT , beta blockers in CHF etc. It is ironical , we are in the era of rediscovering common sense with sophisticated research methodology .What our ancestors know centuries ago , is perceived to be great scientific breakthroughs . It takes a pan continental , triple blinded randomised trial to prove physical activity is good for the heart .(INTERHEART , MONICA studies etc) .
Medical profession is bound to experience hard times in the decades to come , unless we look back in time and “constantly scrutinize” the so called scientific breakthroughs and look for genuine treasures for a great future !
Common sense protects more humans than modern science and it comes free of cost too . . .
Exercise stress test ( Also called treadmill test ) is an important investigation not only in patients with suspected CAD but also in established CAD . In the former group , it helps us to exclude CAD in patients with chest pain and in the later group , it helps us to assess functional capacity , risk stratification and to detect any additional ( New or residual ) ischemia.
Stress test being a physiological test , has a huge advantage of assessing the adequacy of myocardial blood flow without even knowing the coronary anatomy , while Coronary angiogram (CAG) has a zero physiological value* in spite of excellent assessment of the coronary anatomy !
It is an irony , in the assessment of angina we are expected to assess the physiological adequacy of myocardial blood flow , we have kept coronary angiogram as a gold standard over and above the much neglected physiological stress test.
Of course, the limitation of stress test is that , it has only 75% specificity( to rule out CAD ) and about 80% sensitivity (To detect CAD ) .In simple terms stress test is likely to miss 20% times to miss a CAD in patients with CAD and 25% of times falsely diagnose CAD in patients without CAD.
In the above statistics , coronary angiogram was considered gold standard . The problem with this data is that , CAG is not the real gold standard ,but it was nominated as a gold standard . We now know normal coronary angiogram is not equivalent to normal coronary arteries and vice versa.
While both test have limitations , it is logical to believe CAG has an edge over stress test since it visualises the anatomy. But , once an obstruction is demonstrated by CAG, stress test scores over in assessing the physiological impact of the lesion.
Is a 70% LAD lesion significant or not ?
Stress test will give vital information to answer this question.If this patient performs 10-12Met exercise without symptoms it means , the obstruction is not impeding the flow even during stress. He may do well with medical therapy.
What does a positive stress *mean for the patient and for the physician ?
(* A false positive EST in LVH, anemia, baseline ST shifts are included in discussion )
A positive stress test with or without angina at low workload <5 METS indicates very significant obstructive CAD either in left main , or proximal LAD/LCX. They should getimmediate CAG.
A positive stress test at load 5-10METS is again significant and patients should get early CAG
A positive stress test with angina at good work load >10-12 mets would indicate insignificant or minimally obstructive CAD.
A positive stress test at the peak of exercise at good work load > 10-12METS without angina could indicate a false positive or very minimal CAD.
For the physician , the proper way of interpretation should be , the fact that a person performs 10-12 METS indicate the myoacardial blood flow would be more than adequate in most life situations. Knowing the coronary anatomy serves no purpose here, as no revascularisation will be attempted even if he is going to have a significant CAD ( Which again , is also highly unlikely ) .He should be managed with appropriate lifestyle (Diet, activity, relaxation ) anti anginal drugs, aspirin , good lipid control and plaque stabilisation with statins .
Can a patient with critical left main or proximal LAD perform >10METS in exercise stress test ?
No , large clinical experience (Also refered to Class C evidence by ACC/AHA!) indicate no patient with critical left main or equivalent disease can perform 10 METS excercise
While , EST may be less hyped investigation, but it is the only noninvasive test , ( that too , simple and cheap ) that can rule out * a significant left main or equivalent almost 100% correctly .
Now that, the results of COURAGE and BARI 2D have clearly indicated medical therapy is best form of management in chronic CAD , ( except in severe obstructive CAD in vital locations) a positive EST at > 10-12Mets , has absolutely no indication* to for doing a CAG.
*Some would advocate a policy of doing a CAG as a baseline investigation in all patients with positive EST to know the coronary anatomy and will not proceed onto revascularisation if there is insignificant lesions.
Further , real life experience has taught us , routine CAG in these patients
Increases patient anxiety as he is given a report with a diagram of obstructed heart vessels
Leads to multiple cardiac consultations
Divergence of opinions
Finally end up in the likely hood of a inappropriate revascularisation for a insignificant distal CAD.
Final message
Every patient, who has positive stress test , ( Please note , it could even be true positive ) need not undergo CAG . Most interventional cardiologists could feel otherwise , but one should also remember , There is one more role for the interventional cardiologist ie , to intervene when inappropriate interventions are done to their patients.
NSTEMI constitutes a very heterogeneous population .The cardiac risk can vary between very low to very high . In contrast , STEMI patients carry a high risk for electro mechanical complication including sudden death .They all need immediate treatment either with thrombolysis or PCI to open up the blood vessel and salvage the myocardium.
The above concept , may be true in many situations , but what we fail to recognize is that , STEMI also is a heterogeneous clinico pathological with varying risks and outcome ! Let us see briefly , why this is very important in the management of STEMI
Management of STEMI has undergone great change over the past 50 years and it is the standing example of evidence based coronary care in the modern era ! The mortality , in the early era was around 30-40% . The advent of coronary care units, defibrillators, reduced the mortality to around 10-15% in 1960 /70s . Early use of heparin , aspirin further improved the outcome .The inhospital mortality was greatly reduced to a level of 7-8% in the thrombolytic era. And , then came the interventional approach, namely primary PCI , which is now considered the best form of reperfusion when done early by an experienced team.
Inspite of this wealth of evidence for the superiority of PCI , it is only a fraction of STEMI patients get primary PCI even in some of the well equipped centers ( Could be as low as 15 %)
Why ? this paradox
Primary PCI has struggled to establish itself as a global therapeutic concept for STEMI , even after 20 years of it’s introduction (PAMI trial) . If we attribute , lack of infrastructure , expertise are responsible for this low utility of primary PCI , we are mistaken ! There are so many institutions , at least in developing world , reluctant to do primary PCI for varied reasons.( Affordability , support system , odd hours ,and finally perceived fear of untoward complication !)
Primary PCI may be a great treatment modality , but it comes with a inherent risk related to the procedure.
In fact the early hazard could exceed the potential benefit in many of the low risk STEMI patients !
All STEMI’s are not same , so all does not require same treatment !
Common sense and logic would tell us any medical condition should be risk stratified before applying the management protocol. This will enable us to avoid applying “high risk – high benefit” treatments in low risk patients . It is a great surprise, the cardiology community has extensively researched to risk stratify NSTEMI/UA , it has rarely considered risk stratification of STEMI before starting the treatment.
In this context , it should be emphasized most of the clinical trails on primary PCI do not address the clinical relevance and the differential outcomes in various subsets of STEMI .
Consider the following two cases.
Two young men with STEMI , both present within 3 hours after onset of symptoms
ST elevation in V1 -V6 , 1 , AVL , Low blood pressure , with severe chest pain.
ST elevation in 2 ,3, AVF , hemodynamically stable , with minimal or no discomfort .
In the above example, a small inferior MI by a distal RCA occlusion , and a proximal LAD lesion jeopardising entire anterior wall , both are categorized as STEMI ! Do you want to advocate same treatment for both ? or Will you risk stratify the STEMI and treat individually ? (As we do in NSTEMI !)
Current guidelines , would suggest PCI for both situations. But , logistic , and real world experience would clearly favor thrombolysis for the second patient . Does that mean, the second patient is getting an inferior modality of treatment ?
Not at all . In fact there is a strong case for PCI being inferior in these patients as the risk of the procedure may far outweigh the benefit especially if it is done on a random basis by not so well experienced cath lab team. (Note : Streptokinase or TPA does not vary it’s action , whether given by an ambulance drive or a staff nurse or even a cardiologist ! .In contrast , the infrastructure and expertise have the greatest impact on the success and failure of PCI ) Final message
So , it is argued the world cardiology societies(ACC/ESC etc) need to risk stratify STEMI (Like we do in NSTEMI ) into low risk, intermediate risk and high risk categories and advice primary PCI only for high risk patients.
This is a 15-year-old post about LVH, written in 2008. Few of my colleagues, now agree with this, still hesitate to oblige in the open, suggesting it is too good to be true! Re-posting it for your own assessment. Surprised, why cardiology community didn’t consider this observation worthy to pursue.
Advantages of Left ventricular hypertrophy (LVH)
Left ventricular hypertrophy is one of the most common clinical cardiac entity.It is recognised either by ECG or echocardiography.LVH has a unique place in cardiology as it can imply a grossly pathological state or a marker of healthy heart as in physiological hypertrophy in athletes.
Logic would suggest, in this era of stem cells and nano medicine , every muscle fibre in ventricle is worth in gold !. So when the nature provides an extra reserve of myocardium in the form of LVH one should welcome it , if otherwise not harmful.
Is LVH due to systemic hypertension benign ?
Not really, LVH has been shown to be an independent cardiac risk factor. (The famous Framingham study)Further LVH can result in diastolic dysfunction and the risk of cardiac failure increases.
But in spite of these observations, an astute clinician with considerable experience will appreciate , patients with LVH fare better during an acute coronary syndrome !
This has been a consistent clinical observation . (Shall we call it as class C . ACC /AHA evidence ? )
Is LVH an asset during ACS ?
A hypertrophied heart takes ischemic injury very easy , it doesn’t really hurt much . Another possibility is that in LVH myocytes are relatively resistant to hypoxia .
Patients with LVH rarely show significant wall motion defect following an STEMI.This is probably because the full thickness transmural necrosis is almost never possible even if extensive MI occurs.
This is also reflected in ECG as these patients rarely develop q waves in following STEMI .
Persistent ST elevation and failed thrombolysis is very uncommon in pateints with LVH.
LVH provides a relative immunity against development of cardiogenic shock . It requires 40% of LV mass destruction to produce cardiogenic shock.This can rarely happen in LVH. In a long term analysis we have found none of the patient with LVH developed cardiogenic shock following STEMI.
LVH patients are also protected against development of free wall rupture.
Concluding message
“Lack of published evidence is the weakest evidence to dismiss a true myth”
LVH , either pathological or physiological, has a hitherto unreported beneficial effect.It acts as a myocardial reserve and helps limit the impact of STEMI.
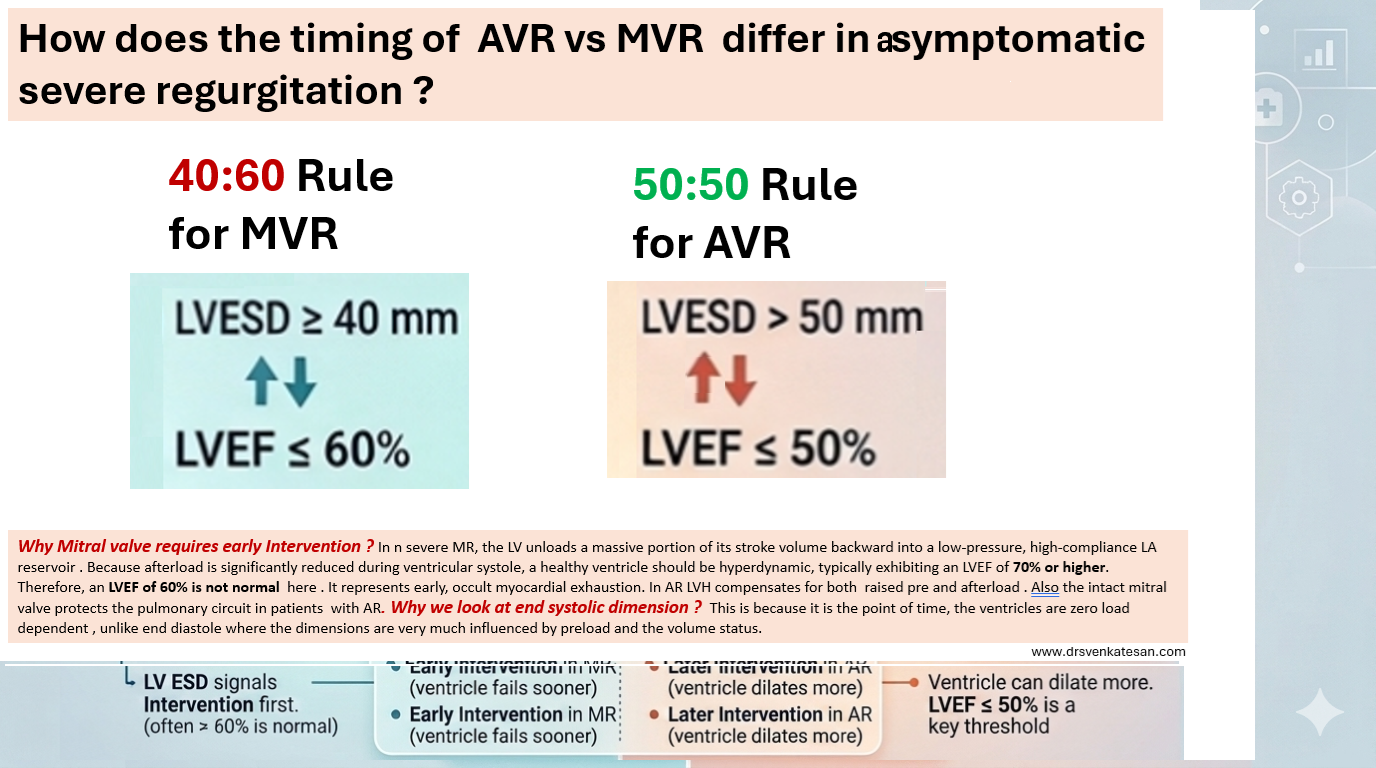
Timing of AVR and MVR in AR and MR has always elicited huge discussion in cardiology literature. Mind you, if the patient is symptomatic and there is LV dysfunction, it is absolutely easy to make a decision.Here, the question of timing doesn’t arise at all. (Of course, the symptoms and LV dysfunction should be confirmed to arise because of valve disease, not because of any other systemic disease, or LV dysfunction might be due to associated CAD. *I know a women who got her leakinging mitral valve replaced because she developed symptoms of dyspnea due to anemia .
Timing becomes a big issue only in patients with no symptoms at all. Some cardiologists put them on a treadmill. It is controversial, as anyone will develop symptoms. But , somehow, we should make it sure, patients are truly asymptomatic.
For long, we relying on some gospel echo parameters. I don’t how good they are. But , no one really knows,how and when the onset of LV dysfunction would be , and how it will progress. But, we are bound by the guidelines , as on today. There is some critical difference between the echo parameters , based on we intervene.
For mitral valve the threshold is lower. It needs early MVR for same degree of regurgitation as AR. It is proposed by the author for the benefit of fellows to easily remember the cut offs. It may be called as the 40:60 rule for MVR and 50:50 rule for AVR. The former denoting LVESD and later referring to LV EF %. The difference in echocardiographic thresholds arises because the two lesions cause fundamentally different hemodynamic loads on the left atrium and ventricle .(Read the legend in Image)
Final message
With mortality and morbidity for valve replacement steadily falling, it is likely more and more patients will be taken for surgery early. Of course, intervention guys are raring to go with percutaneous TAVR and TMVR, so the thresholds are expected to fall.
What is the brief conclusion of this important study from EUROPACE ?
This meta-analysis aggregates data from 6 randomized controlled trials involving over 7000 patients to answer a burning question. Should we aggressively plug LAA in lieu of OAC or DOAC in AF ?
The short answer from this meta-analysis is a resounding “no” if our primary clinical goal is preventing ischemic stroke
For all those cardiologists and physicians who have huge trust on LAA closure for AF , this study delivers a remarkable reality check:
The Stroke Incidence : The very purpose these devices are implanted is reduce it. But what happens ? Patients randomized to LAA closure suffered a 41% higher relative risk of ischemic stroke or systemic embolism compared to those on oral blood thinners.
The Harm : In a 3-4-year follow-up period, the Number Needed to Harm (NNH) may not look significant. For every 100 patients given a shiny new implant, one additional patient will experience a stroke that a simple daily pill could have prevented.
The Bleeding Trade-off: To its credit, LAAC successfully reduce the bleeding risk associated with OAC/DOAC
Will this study change the FDA approval and guidelines ? What will be the future of LACC ?
No, Absolutely not. FDA is unlikely to react. It reviews devices based on their safety profiles for specific, indicated populations. Because these devices successfully reduce bleeding rates for patients with an absolute contraindication to blood thinners, their approval is legally and clinically sound.
The medical gadget eco-system works seamlessly . A device manufacturer proves that a LAA plug stops bleeding in a high-risk group. The device gets approved. Most of us fall for it and naturally shifts toward “liberal usage” as an easy, high-revenue alternative for patients who just don’t feel like swallowing a pill every day.
Final message : LAA closure device is not really a useless device , but you need to use, it less .
With an estimated 400,000 implanted annually , it is too hard for us to say LACC is useless. The future will inevitably bring next-generation devices with fancier anti-thrombotic coatings or redesigned plugs. Meanwhile, thousands of low-risk patients will continue to undergo unnecessary procedures , forcibly accepting the risk of increased stroke for the sake of convenience & glamor.
Which one of the following is least important to become great doctor ?
A. Compassion & Caring
B. Sincerity & Hard work
C. Knowledge & Skill
D.Honesty & Integrity
Trying to answer
Yes I agree, It is brutal to frame such a question. If healing, and taking care of the suffering mankind, is the primary purpose of the noble profession , after 4 decades in to the Noble profession, realised a possible truth .Knowledge and skills are vital, but sadly lags behind the other three by considerable distance.
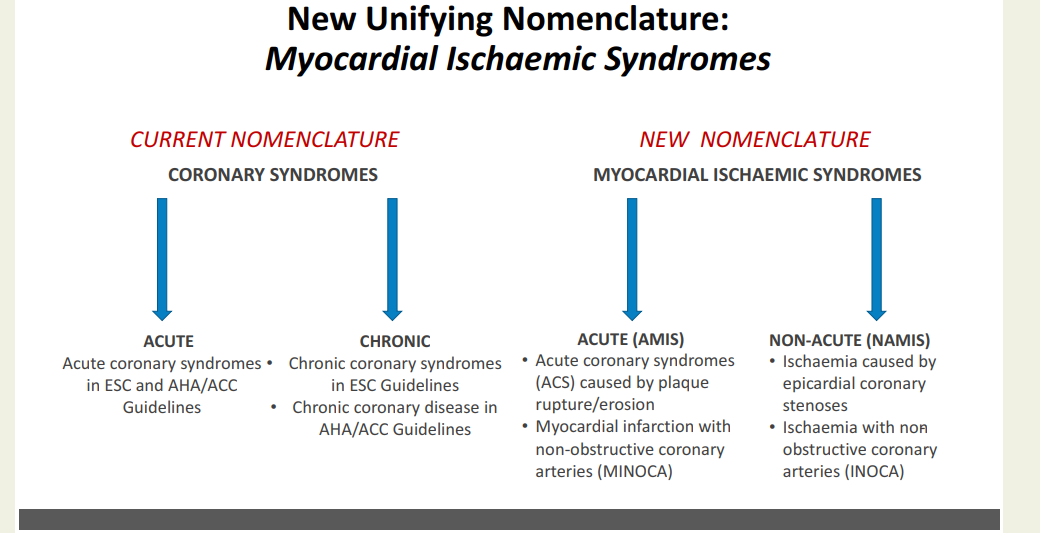
CAD : It is been called IHD, CCD, CAHD, CCS, etc. Now there is a new proposal from European Heart journal (with an Impact factor of 48 ) to change the nomenclature of chronic coronary syndrome to NAMIS : Non acute myocardial Ischemic syndrome (Ref 1)
What is the purpose & need to change the current terminology ?
The proposed AMIS and NAMIS classification shifts the clinical paradigm from coronary anatomy to myocardial function. For decades, terms like “coronary artery disease” overemphasized epicardial stenosis, neglecting the reality that ischemia frequently occurs without structural blockages. Data shows that up to 40% of symptomatic patients lack macroscopic obstructions, suffering instead from microvascular dysfunction, vasospasms, or myocardial bridges. This new term NAMIS can bring in the phenotypes like INOCA and MINOCA into the CCS without any conflict. Further, replacing vague adjectives like “stable” or “chronic” with “non-acute” reflects the high long-term residual risk of cardiac events. I also think, this new framework is meant to unify the European and American guidelines, where they use differing terminologies.
Counter Point : Do we really need this ?
Purpose of any new classification is , it should have a clear impact on patient management. But, we often find, scientific committees periodically take pride in changing the nomenclature akin to make a academic fashion statement .Within a few short years, we migrated from stable CAD to SIHD, switched to CCS , CCD etc . The fact is , for the patients it is the same angina for which they seek relief. They simply don’t bother whether doctor label their condition a syndrome or disease .
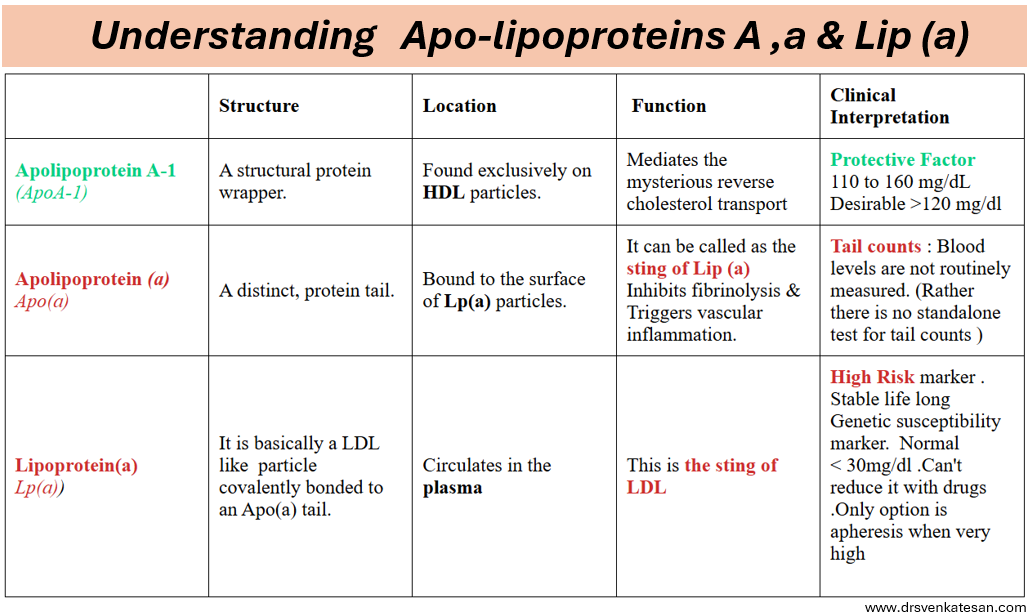
It is an irony, we call the lipids as chief villains in the genesis of atherosclerosis and CAD. The fact of the matter is, it is the protein component that hides among the lipid jelly, with multiple folds and stinging tails, that ultimately help the LDL to penetrate the intact endothelium . These are called , apo-lipoprtiens. The fate of lipid molecules is determined by these apparently humble looking proteins .It must also be noted the even the goodness of HDL vanish if its apo-liprotein fails to co-operate . The Apo proteins are labeled differently in each sub fraction of lipids. Its Apo A 1 in HDL Apo B 100, in LDL and Apo C in VLDL.
Playing with English Alphabet A
Scientists can be casual , though not intentional when naming newly detected molecules. The major nomenclature issues are with Apo A , Apo a , Lip a These three entirely separate proteins with nearly identical names, should not be confused with. A subtle shift between a lowercase letter and a capital letter completely changes the meaning, taking us from a highly dangerous cardiovascular risk factor to a healthy, protective one.
Apolipoprotein A : This is a highly beneficial protein that defines the HDL function.(Ofcourse one must remember too much of HDL can be toxic as well .In fact when it exceeds 60 mg ,it will become dysfunctional, rather harmful.This is the U curve phenomenon of HDL)
Apolipoprotein(a) : This is the sticky, genetically fixed protein tail found only on Lipoprotein(a). It promotes blood clotting and triggers arterial inflammation.
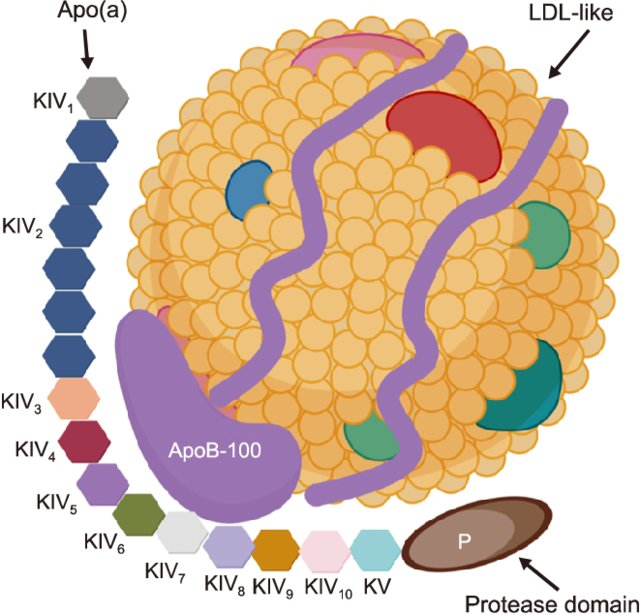
Lp(a) : It is formed when a single Apo(a) protein tail binds to the Apolipoprotein B-100 (ApoB) wrapper of a standard LDL like particle. Because of this hybrid structure, Lp(a) possesses dual pathogenic properties. LDL core delivers cholesterol into the arterial wall, while the attached Apo(a) tail promotes localized inflammation and thrombosis . Lp(a) plasma levels are strictly determined by inheritance and remain highly stable throughout an individual’s life.
Lipoprotein(a) structure. Lp(a) is composed of two parts: one part is low-density lipoprotein (LDL)-like particles with apolipoprotein B100 (apo-B100), and the other part is the stinging tail apolipoprotein a [apo(a)]
Among the above three molecules, lipoprotein(a) is the celebrated one kept in the limelight. It is strongly determined by genetics and is a predictor; rather, we can call it a marker of LDL virility (like Apo B 100). It is entirely produced in the liver, its level is claimed to be static lifelong. Obviously, it cannot be true, as it would heavily dependent on liver function. Further, different vendors have come into the market with this, and they have different normal ranges.
Final message
When reading the lipid molecules, please focus on the English . A capital A vs. small a makes a huge difference between harming and healing the patient. Of course, we must be thankful, as of now, we have don’t have no small b or small c Apolipoproteins in lipidology.
India is sort of burning, with students on the streets for exam reforms.The problem started with the leakage of question paper for National Entrance and eligibility test for medical college( NEET) Government is on the back foot. The prime minster has come out, assured the students and their concern will be taken care of. Yes, it is true greedy cartels are exploiting the system. But, we are ignoring a big hidden moral failure in the whole issue.
However, It is very convenient to march through the streets pointing fingers at the state, but blaming the government alone is not enough to fix a rotting system. We love to demand absolute structural perfection from institutions while completely ignoring the mirror of reality. It is us, the public that fuel and maintain the corruption supply chain through a collective, desperate willingness to bypass merit at any cost.
Let’s be honest, even a un-breachable testing infrastructure cannot save an education system where parents and students are actively looking for illegal shortcuts. When families willingly treat leaked question papers as a premium commodity, they are not victims they are the core investors funding the black market. I wished, I could find at-least one banner conveying this fact too.Unfortunately, it can never happen.
True reform cannot happen through government orders alone. It requires a brutal confrontation with our own societal hypocrisy and a complete dismantling of the demand side of corruption.
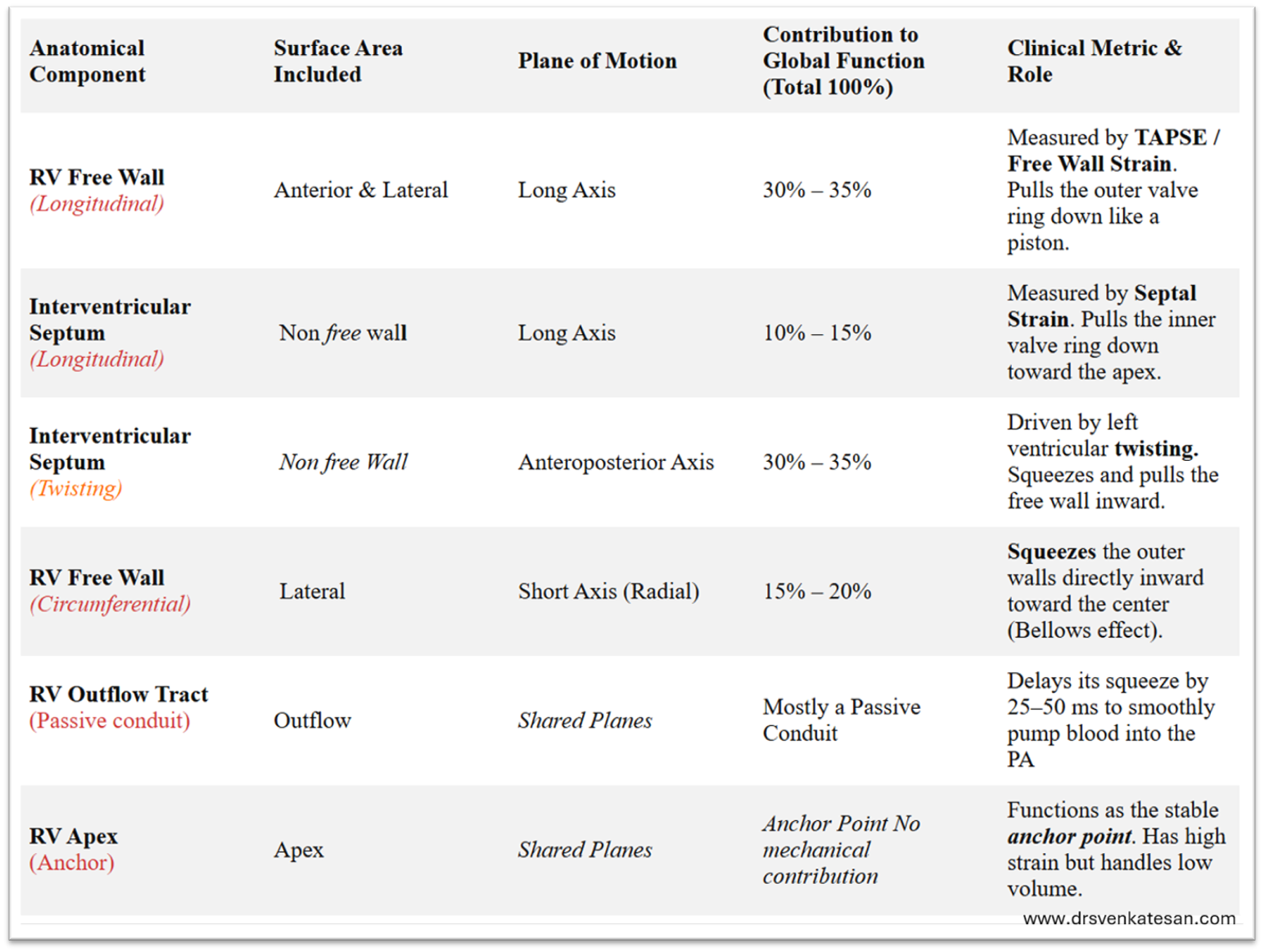
TAPSE the most celebrated RV function index misses significant Right Ventricular (RV) dysfunction in an estimated 30 to 50% of patients. ( when relying solely on it).It fails to detect underlying impairment because it only measures the longitudinal shortening of the RV base, largely ignoring global chamber contraction.
Mechanism attributed to the unreliability of TAPSE
Ventricular Interdependence: The RV motion is influenced by left ventricular function by the shared IVS contraction.
Chronic Volume or Pressure Overload: Conditions like severe tricuspid regurgitation or pulmonary hypertension cause the RV to alter its contraction geometry. This leads to “pseudo-normalization, of TAPSE” it remains >1.7 cm despite dysfunction.
Post-Cardiac Surgery: In patients who have undergone procedures involving pericardiotomy, TAPSE often drops drastically as post pericardiotomy the RV radial function exccedds longitudinal
Loading Dependency : TAPSE is highly influenced by preload and afterload conditions.
The following table summarises the various components and it’s contribution to RV contractility.
*Contrary to the popular belief, there is overlap between free wall contraction and longitudinal contraction. In fact, there is no clear definition for RV free wall. Logic tells us, any part of RV which is not formed by IVS can be considered free.
*Importantly, Longitudinal contraction has a two components free wall as well as a septal axis. TAPSE measures only lateral or free wall component of longitudinal function. It is less influenced by septal long axis function.
*The long axis function of RV is influenced indirectly by the LV function also as both AV valves are attached to same ring.
*If we want to assess pure RV function the best index is RV free wall circumferential or radial contraction or strain.
*In various clinical situations like PH or acute pulmonary embolism the pressure distribution is non-uniform making the assessment of RV function difficult. Fractional shortening of area is a fair index.RV wall motion abnormality can be subtle yet a serious marker of RV dysfunction.
Final message
RV function assessment is complex and often incomplete. The habit of relying only on TAPSE, is not a high quality scientific practice.
Postamble : Apart from the contractile function, we don’t know at what RV pressure RV begins to dilate. This is different in acute vs chronic elevation. We also don’t know which patient will show RV hypertrophy, and which group prefers dilation. May be, all these are academic and has little significance at the bedside. However understanding this is essential to assess the response to RV inotropes and newer RV assist devices.
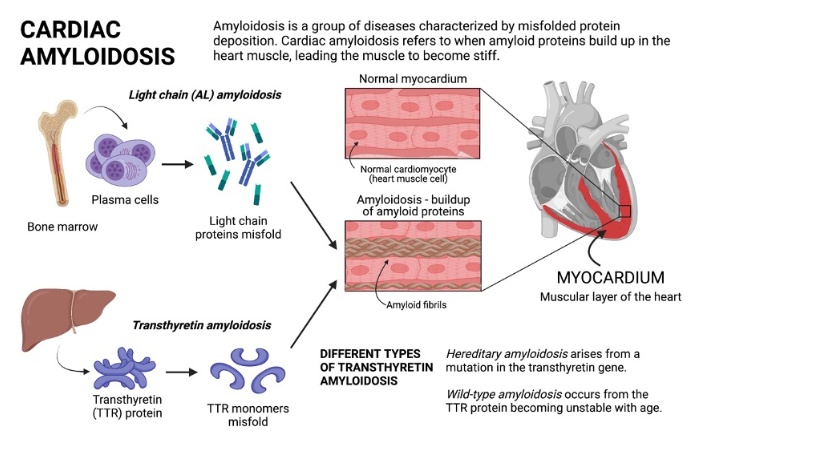
Amyloidosis is a proteostatic disease , meaning a progressive disorder of extracellular deposition of insoluble protein fibrils in tissues.It affects , brain, kidney, nerves and almost any organ.Crucially, amyloid is an interstitial disease, accumulating strictly in the spaces between cells rather than inside them. This interstitial buildup exerts physical pressure, alters tissue architecture, and finally invading the cell and hence the organ function.
The primary culprit is a normal transport protein transthyretin (TTR) (same as prealbumin) It is synthesized in the liver as a stable, four-part tetramer structure that safely circulates in the blood. Under stressful or aging conditions, this tetramer destabilizes unstable monomer pieces. These monomers undergo misfolding, polymerizing into rigid cross-beta-sheet amyloid fibrils. These abnormal ATTR fibrils escape cellular degradation.
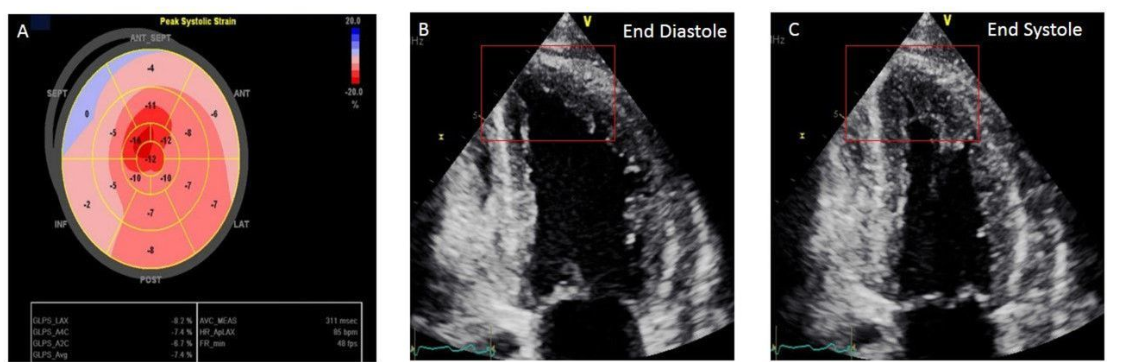
Cardiac amyloidosis
Cardiac amyloidosis , presents as mainly as restrictive cardiomyopathy, but can be seen in any chronic heart failure associated with LVH, especially in Aortic stenosis, where it can involve both the valve and myocardium.There are multiple reasons why we diagnose amyloidosis more often than before. But , one thing is sure, it is not due to increasing incidence in the population , but more of a high awareness and availability of advanced cardiac imaging .
Image source : Agha AM,. Role of cardiovascular imaging for the diagnosis and prognosis of cardiac amyloidosis. Open Heart. 2018;5:
What is the confirmatory test for Amyloidosis ?
It was classically diagnosed by tissue biopsy with Congo red staining, showing “apple-green” birefringence under polarized light microscope. Mass Spectrometry, Immunofluorescence is then used to decode the protein composition. Currently , with typical patterns of cardiac imaging we can diagnose with confidence without biopsy. While echocardiography is good enough , MRI and technetium-99m pyrophosphate scans are crucial.
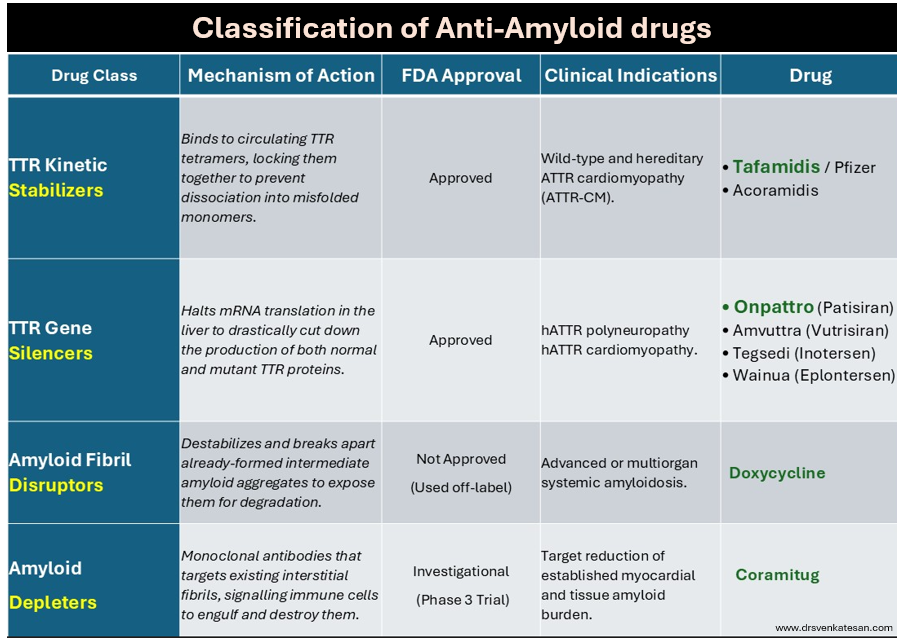
What are the specific treatment option for amyloidosis ?
Until recently, Amyloidosis, has been considered as irreversible degenerative disease .Now we have strategies to reduce progression or even regress the Amyloid deposition. Many drugs are still being studied with varying success.
Following table summarise the different pharmacological modalities to tackle Amyloidosis.
Final message
A limitation of currently approved anti-amyloid medication such as Tafamidis or Onpattro , is that it cannot be reversed and only be prevented.Emerging technologies like monoclonal antibody depleters hold promise to actively clear out existing deposits, potentially turning it to a truly reversible condition. Chronic fibrotic pathways from triggered fibroblasts are closely linked to Amyloidosis. Hence, antifibrotic drug research should go hand in hand with Amyloidosis.
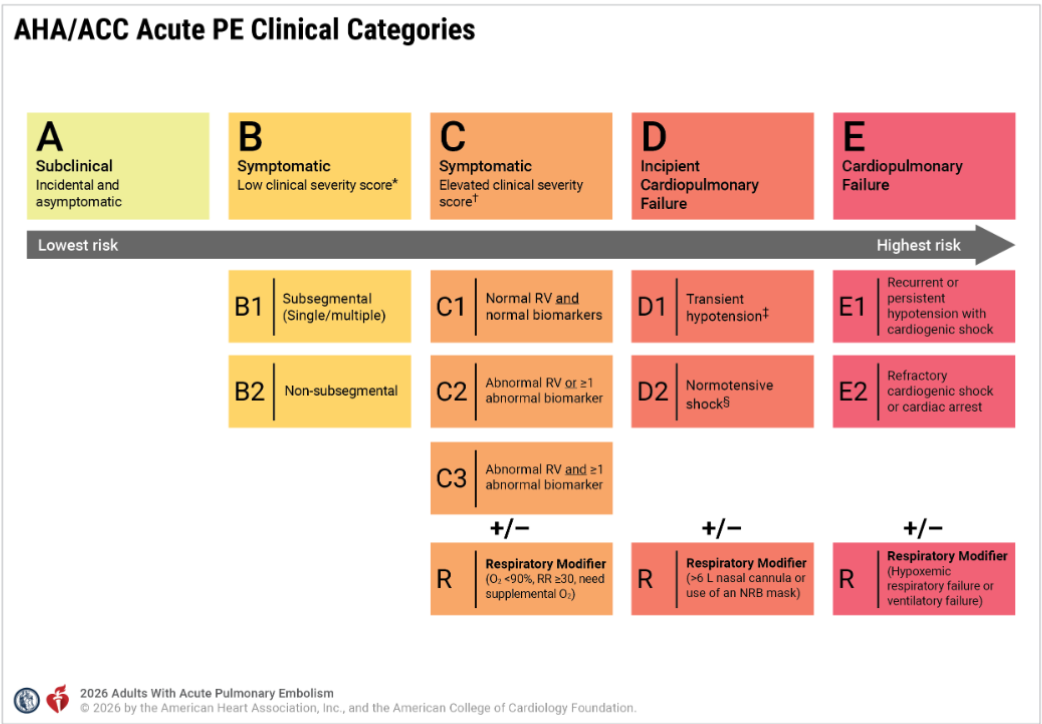
Pulmonary embolism continues to be an intriguing entity, both in the diagnosis and management. The spectrum is wide, from a clinically insignificant, or totally unrecognized episode to a massive cardiopulmonary event causing sudden death. Similarly, treatment can either be conservative (even sending the patient home ) or lead to aggressive cath lab intervention.
The task of PE risk stratification
Obviously, risk stratifying is the mainstay in the management.The fact that we are grappling with multiple risk stratifying scores like PESI, simplified PESI or HESTIA expose our limitations. To segregate , low and high‑risk categories do not demand much expertise. It is the intermediate‑risk group that plays havoc in the ER. It is based on RV function and biomarkers like troponin and D‑dimer. But it was soon realised clinical parameters like blood pressure and hemodynamic stability are the more powerful markers of risk.
However,the reality is, many patients in the intermediate‑risk group are rushed to the cath lab, either due to overestimation of risk or fear of potential escalation to high risk. A third reason,is often non‑academic, it’s done for showing our expertise.
Now, to solve the puzzle of intermediate risk, we have created two new subcategories, C and D. ACC/AHA has been very careful in defining and labeling the entities. Still, there are a lot of gaps that need to be fixed.
In this post let us confabulate few aspects of the new grading of PE and in particular the curious case of D 2 shock .
series of iFAQ ( infrequently) asked questions will from the basis of this discussion
Does category C to D progress in a sequentially worsening hierarchy?
Though it looks that way, the clinical presentation rarely follows a sequential order.
Why is BP is not given adequate weightage in Category C?
A normal blood pressure is a mandatory baseline requirement to enter Category C. However, BP is an important factor used in the clinical severity assessment (PESI etc) .It is not clear why , the committee did not explicitly use the term Category C with reference to BP.
Why is the word “symptomatic” missing in Category D?
The word “symptomatic” is deliberately omitted from the title and subcategories of Category D in the 2026 AHA/ACC Pulmonary Embolism guidelines because symptoms alone are no longer a differentiating factor at these higher levels of severity. Alos, the patient needs to be alert, to tell the symptoms.
Does that mean symptomatic Class C is less risky than asymptomatic Class D?
Yes. A symptomatic patient in Category C is at a significantly lower risk of dying or collapsing than a patient in Category D.A patient in Category C might feel worse because they are aware of their chest pain. A patient in Category D may not complain of pain at all, perhaps because they are in altered sensorium.
What is D2 shock, and when and how do we diagnose it?
First, the patient must fulfill the baseline criteria of Category C, which includes right ventricular dysfunction and positive biochemical parameters of either Troponin or NT-Pro BNP. Then, they must have at least one parameter to confirm shock. Under Category D, the term normotensive shock defines the D2 category, where the blood pressure is normal.
The signs of shock include:
Lactate greater than 2 mmol/L.
Evidence of acute kidney injury, meaning urine output is less than 0.5 mL/kg/hr.
Altered mental status changes.
A cardiac index less than 2.2 L/min/m2.
A mean arterial pressure less than 60 mmHg.(In D2 shock the MAP more than 60 mmhg)
Is elevated lactate mandatory to diagnose D2?
No. Any single criteria from the above list is enough. Oliguria alone or even altered mental status is sufficient.
Can D2 shock be diagnosed based only on altered sensorium?
Yes. it is possible to diagnose Category D2 based only on a vague, mild, or temporary change in mental status .This carries a huge risk of falsely classifying a stable Category C patient into the more critical Category D. To prevent this error, the 2026 AHA/ACC guidelines has strict definition of Category D2, ie the altered sensorium must be profound and persistent.
Why Category D1 patients can show a fall in BP, while Category D2 has normal BP?
In PE, the right heart is overwhelmed by the acute rise in RV afterload, causing a short term drop in the volume of blood until the RV recovers. This is the mechanism of fall in BP D1.In Category D2, the blood pressure stays completely normal (90 mmHg or higher), but the patient may be in ongoing organ shock spiral. In D2 the RV is failing just like in D1, but the patient’s sympathetic response fires at it’s peak with maximum vasoconstriction to sustain the BP and life.
Why D2 shock sounds a mystery ?
It may look implausible that a patient in D1 can have low blood pressure, but when they worsen, they seemingly gain blood pressure to reach D2 and get the tag of normotensive shock. In the bed side this is not true. The hidden clinical reality is, D1 and D2 are not meant to be viewed as sequential, worsening hierarchical stages. A patient can move from Category C to D1 or D2 directly, and a direct jump from Category C to Category E is also possible without spending any time in Category D.
Dynamics of the C-D-E categories
It becomes problematic to have the term normotension in the title itself in D2 . This implies ,a patient with hypotension and underperfusion should exit from D2 shock. This could mean a worsening patient paradoxically enters Category D1 or Category C or E. To be precise, a fall in blood pressure represents is really a sign of worsening or not is debatable and decided on patient to patient basis. Also both category C will also feature a normal blood pressure. This can be mixed up with D2 if organ perfusion markers like oliguria occur transiently. This trichotomy between hemodynamic stability, organ perfusion , versus respiratory stability needs to be addressed. The PERT team need to be vigilant on this asseement.
Do we need to sub classify D2 shock ?
In realistic observations, the most common cause of normal BP in D2 shock is the intensive treatment these patients receive with RV inotropes and systemic catecholamines. Perhaps we may need to add another rider to Category D2, such as Normotensive with drug support versus normotensive without inotrope support. This would help us know the exact direction in which these patients will progress.
Can Category C3 be riskier than D2?
This is tricky and indeed seems possible . Category C3 can exceed the morbidity of Category D, especially when it features the respiratory modifier as C3R. It must be recalled that both the C and D categories present with right ventricular dysfunction and positive cardiac biomarkers, but their primary organ failure differs. A Category C3R patient experiences an acute oxygenation crisis. Conversely, a Category D2 patient, even with normal lactate, suffers from occult circulatory shock (an adequately functioning liver can clear the lactate efficiently.) Though C3R appears more dramatic at the bedside due to the need of respiratory support , Category D2 carries a higher mortality.
Final message
“It looks like treating patients with PE is much easier task than risk stratifying them“
Pulmonary embolism management is a fierce fight between the right ventricle, the occluded pulmonary arteries and the lungs.The first 48 hrs is crucial. RV shock incidence rapidly reduce after this time window. We realised very late, the total thrombus burden actually has a poor correlation with the final outcome. Most episodes of PE can be managed medically.
Balancing pharmacological lysis versus catheter-based lysis requires a very delicate skill. While most patients are eligible for standard lysis, only a very few truly benefit from catheter-based therapies. The rate of RV failure and mortality drops dramatically once the right ventricle rises to the challenge. Therefore, there is no clinical point in doing a catheter-based lysis if the blood pressure is normal and the right ventricle is already recovering.
Finally and most importantly, the alarming entity D 2 (Normotensive shock) should not cause unnecessary panic. If the, saturation and RV function remains good or shows signs of recovery , catheter based modalities can be avoided.
“Medical care is sought after and delivered with all sincerity and kindness. It is never meant to be sold over the counter” My mentor and respectful professor used to tell us, many decades ago during our undergraduation days. That was a bygone era. Forget it, let us come to the real world.
This ad came two days ago in a India’s leading daily :The Hindu
With all three limbs of the medical profession, namely patient care, teaching, and medical research, under the clutches of commerce and industry, there is no surprise at all, to find this ad in the mainstream media.
How big is the AF burden ?
Atrial fibrillation is a common arrhythmia of the elderly. In that sense, it is more prevalent in the western population where life expectancy is high. AF is more of a nuisance arrhythmia in an otherwise normal heart, which requires stroke prevention strategies like antiplatelet agents or OAC/DOACs. In a hemodynamic perspective it is largely benign arrhythmia , 95% of which can be managed with simple rate modulating drugs like Digoxin and Beta blockers .The costly and often riskier catheter based rhythm restoring modalities still have questionable value except in a fraction of the AF population.
What could be the aim and intention of the above advertisement?
Big companies want to sell complex medical devices and procedures for AF directly to the public.The funny thing in the ad is , while India is grappling with the task of providing basic health amenities like ECG machines in every primary health center , yet this ad expresses serious concern about the low penetration of a new, cost-ineffective, technology called “pulse field ablation” to treat AF.
Final message
I think, Govt of India should seriously consider banning such adverse health Influencing ads. direct to public.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.