When does the high blood pressure befriends blood sugar and instigates the LDL to initiate the vascular damage? Does it sound like medical astrology? Yes, welcome to a new world of network medicine, polygenic risk score & computational genomics. Experts believe this is going to be the future of medicine.
Dr. Jospeh Loscalzo, Physician-in-Chief Brigham and Women’s Hospital, a leader in the field gives a brief introduction.
How to understand these complex subjects?
We need not bother much in one sense. It’s all made to look complex by big data machines and modern scientific wordplay. It is true, that the power of computing and machine thinking will help us reach hidden secrets in our bodies. However, the bottom line is, If we live a simple. peaceful, worthy, active life we can afford to forget about this sophisticated risk predicting science, which comes loaded with unlimited anxiety. Let the science grow at its own pace.
Imagine the consequence of a powerful artificial intelligence algorithm telling us in advance all the possible future biological adversaries with 100% accuracy.
Final message
Do you believe in astrology, an ancient Indian science? No. Never!
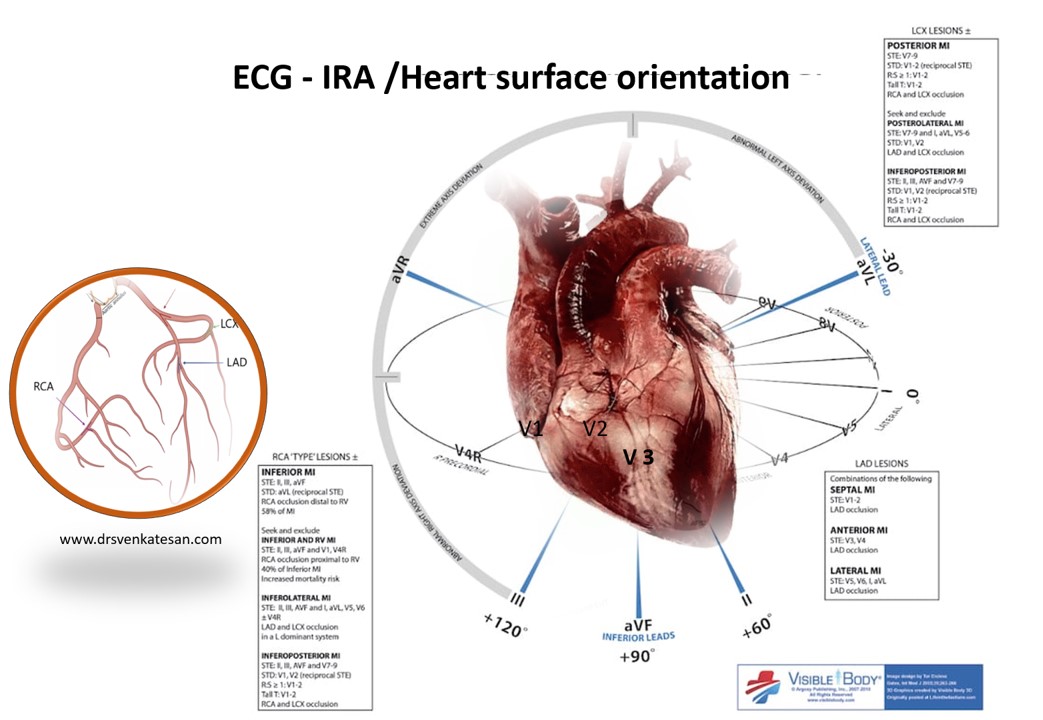
The 12-lead ECG is the single most important investigation that has withstood the test of time for over 100 years. I think it will never lose its relevance in cardiology. However, the traditional sequence of the 12 lead printout could have been a little more user-friendly, especially in its ability to convey the anatomical orientation. Expecting some Innovation in the ECG reporting format.
This illustration helps us to understand, ECG lead orientation, and coronary arterial territory, IRA localization with reference to the various surfaces of the heart. (Courtesy of visible body-modified ) Always remember the heart is an organ, made up by a complex fusion and rolling of bundles of muscles over a fibrous skeleton. It has multiple surfaces. Please avoid calling various surfaces of the heart as walls(Request the young medical students to un-tune their brain, from the inherent tendency to Imagine the heart as a well-demarcated four-chambered concrete structure built with bricks !)
Animated version
Currently, IRA localization with ECG may seem to be a redundant exercise, as we are straightaway seeing the coronaries if taken for primary PCI or at least within 24-48 hrs mostly.
But, IRA localization gives us a rough idea(still useful) of what we are going to deal with during the PCI.
More importantly, multivessel CAD during STEMI can be very significant in the elderly, diabetic, and in women, which can sometimes confuse us about the real culprit artery. (Recanalised IRA vs other chronic lesions). Similarly,
CTOs can masquerade as ATO and vice versa. Here, ECG will come in handy to identify the true culprit.
One useful tip in IRA localization of LAD
Lesions proximal to D1 will depress the ST segment in inferior leads. In other words, if reciprocal ST depression is seen in inferior leads it is most likely a proximal LAD lesion. Paradoxically, in distal LAD lesions, ST elevation occurs in 2,3,AVF. (What may look like a global MI, is in-fact less sinister since it is a distal LAD Infarct)
* The wrap-around LAD* can also mimic distal LAD lesion with simultaneous Inferior and anterior ST elevation. *The wrapping needs to be complete and reach almost the crux (Super dominant LAD ) to cause ST elevation in 2,3, AVF.
Final message
The limitation of surface ECG in localization is real
Multiple IRAs or diffuse lesions, and collaterals all can confound the ECG -IRA correlation.
There can be overlap between large diagonal, Ramus (or even a large OM) when they all try to converge on the curvey and imaginary slope between the anterior lateral wall
Localization of IRA (Rather Angina-related artery (ARA) is a different exercise altogether.
Experienced operators will agree there have been many occasions, where multiple diffuse lessons with delicate collaterals interwoven make IRA identification so difficult, and ultimately primary PCI is abandoned, and the patient returned back into CCU for lysis (Fortunately, Tenekteplace, and streptokinase never need to bother about IRA localisation you know !)
It is likely, that the biggest Impact & influence in current medical research may not come from the IQ of our scientists, their concepts, or the sophistication of the laboratory. Then what? Can you guess? It is the man-made mathematic sub-specality called statistics. We are going to either ratify or reject any research work ( on which we toil) based on the quality of numbers we generate. Such is the critical value of this specialty. Just pause a moment, and think over. How much importance do we give to the credibility and “quality of the interpretation”of any study? We have conveniently left it to our esteemed mathematical colleagues and some other invisible forces for a proxy inference.
I don’t think we will ever find an answer for this. Whether facts are made by statistics or statistics are made by facts ?
In recent times, one technique called propensity matching and scoring is used to conduct medical research where multiple covariables and confounders play.
What does the word propensity mean?
Oxford defines this word /prəˈpɛnsət̮i/ (pl.propensities)(formal) a tendency toward a particular kind of behavior
What is propensity matching in medical research?
In simple terms, it is doing a study without a true control group. It is a statistical gimmick where in we create an Imaginary or virtual patient arm What a way to conduct a scientific study? Those days, if someone suggests a study without a true control arm, it will go straight to the dustbin. (Of course, the concept came into vogue because we can’t have controls for ethical reasons or the rarity of the condition ) We do have many other conventional covariable analytical methods available A well-written reference (Ellicott C. Matthay, SSM – Population Health, 2020,)
Who created this propensity score?
I thought It was a new concept.No, it was proposed by Rosenbaum et al in 1983. (Ref 1) The extreme popularity it enjoys today is unexplainable. I think it is the simplicity, joy of doing a study without a troublesome control population, and the subsequent herd behavior of medical researchers.
Read here the pros and cons
Final message
Only two questions need to be answered before crowning the “propensity score” to glory in the statistical world. 1. Who has the final authority to define, what amounts to a confounding effect? 2, Whatare the statistical chances of missing an important confounder in toto due to baseline ignorance?
Most statistical methodologies are like Holywood movies, some strike gold for no reason in spite of a lot of flaws. A few examples are meta-analysis and non-inferiorly trials. Propensity matching with a synthetic control arm could be a useful methodology in very selected situations. It is unfortunate it has become a fancy tool and doesn’t deserve the wholesome approval for doing away with the true control arm.
Statistics may be great science, but it seems to work fine, only in the absence of continuous, unpredictable biological interference with mathematics.
Lastly, can propensity score take into account of confounding effects of the non-academic mindset of many researchers in senior positions? What shall we do with many important therapeutic guidelines created apparently based on solid evidence created with poorly created virtual (propensity) matches?
Postamble
Experience-based medicine, wild logical guesses, empiricism, and trial of error methods, all these are unavoidable in medical care and research. We have to move ahead with all the uncertainties in-situ and take our patients to a positive destination.
A brief conversation between an elite consultant and his fellow. (Caution: Grade 2 harsh language)
Hey Doc, why is this guy’s name not found in today’s angiogram list? Any Insurance issues?
No sir, he has every requirement. Thrombolysis was very successful, ST has regressed well and it is nearly isoelectric and only T is inverted. His LV function is normal. In fact, I am not able to pick up any WMA.
Aren’t you aware, that being fine is never a contraindication for a PCI ? Which book teach you like that?
No sir, It’s already beyond 48 hrs sir. What is the purpose of knowing IRA status now? If it is open, well and good.If it is partially closed, again little to gain, right?
Don’t expose your Ignorance. … haven’t you heard of the pharmaco-invasive strategy & open artery hypothesis. Always learn to respect science.
But sir, then why does late PCI of IRA in otherwise stable patients come under class 3 recommendation, if I understand the guidelines correctly, it is a contraindication, am I, right sir? But, this patient got stabilized by us still, why he is compelled to undergo another procedure exposing and adding further risk?
That shows your immaturity. Doing an angiogram is never forbidden. It is the inappropriate late revascularisation of IRA that is the issue.
Agreed sir, how confident are we, that we will stop just with an angiogram after visualizing a tempting lesion in either IRA or non-IRA? (My brief experience as a fellow doesn’t tell a fair story)
Now, you are trespassing into prohibited non-academic zones of cardiology practice. Instead, talk about FFR, OCT, multivessel angioplasty, and ( deferred or instant ) complete revascularization. Think like a true scientist don’t get spoiled at a young age in your career with all this ethical stuff.
Final message
Never allow an ACS to stabilize by medical management, if he is otherwise eligible and affordable for a procedure. You are not authorized to do that.
This write up was triggered after encountering a patient who instructed his cardiologist to remove an incidentaly found block in Right coronary artery.
Oftentimes, It is a funny & futile world out there in modern medicine. Revealing the complete truths or accepting ignorance in critical decisions to their patients, make the Doctors feel that, their academic modesty and reputation are at stake.
Still, many patients expect (and think) the doctors to be 100 % transparent and want to understand the nuances of disease better than the doctors themselves. The current fad of online & offline health education for patients is not an accident of technology. Though some benefits exist, I feel, It is an intentionally promoted, maliciously motivated patient empowering movement, trying to disarm the true professionals.
Dear colleagues, always realize, never allow the default ignorance to become patients’ knowledge and ask them to take decisions on behalf of you. (I know, this is diagonally opposite to current principles of the practice of medicine) Fortunately, this issue doesn’t arise in most public hospitals in our country.
This paper was written 30 years ago with great foresight.
So, act with tact. You can’t hide behind the patient’s preferences in deciding the treatment choice. It can be “as unethical as” any activity that goes against the interest of the patients under which we are taking our oath. I don’t, recall anywhere in the Hippocratic oath, that we pledge to listen to the patient’s choice of treatment. (Rather, we assure to work in their interest always)
Final message
Let us sharpen our own skills first. We shall think about how to distill and consume the muddy knowledge emanating from the current mess of premature research spilling all over academia. Don’t try to educate too much to your patients. There is nothing called academic empathy because leaving it to our patients will ultimately end up equivalent to medical negligence.
Forget about the patient-guided treatment menu card. Think about this, if ordering a trendy new medical investigation purely on a patient’s demand is declared as medical negligence, How many doctors on this planet will be left non-negligent.(Stop. then what is a master health check-up? Who is the master ?)
(Hope this write-up is taken from a proper perspective. No intent to create a chasm between patients and doctors relationship )
It all sounds good on paper. The consequence of not listening to our patients, especially if they land up with complications, will look awkward, is it not? So, I always go by patients’ desires.
Patients tend to believe in fancy investigations and machines and not me, what to do?
No, it is wrong. You can’t justify it. Regarding your concern and impact on our reputation, nothing can be done. The medical judiciary desperately needs some reforms, understand the reality to protect us I always tell my patients they have to accept me as a whole. (Do you enter the Aeroplane’s cabin and check the pilot’s mental and physical acumen every time you board a flight. It is trust,.. complete trust, that drives our life right !)
It is true, that medical professionals must be always under a continuous quality*control regimen. The consequences of consulting less shrewd medical personnel, their errors in judgment, the stress of work, patients need to accept* just like a side effect of a drug or a natural history of a disease.
*, Unlike the engineering field, defining & controlling quality in medical therapeutics is a mystery exercise with multiple agendas!
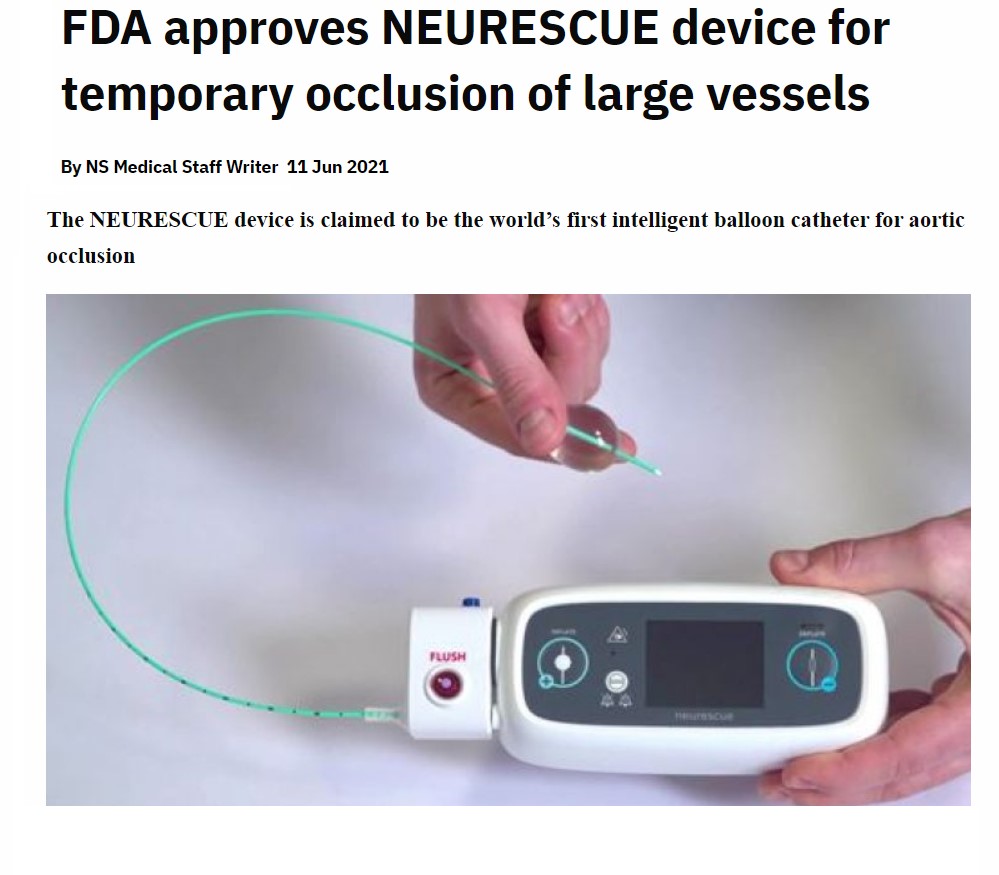
CPR with BLS and ACLS is time tested method of cardiopulmonary resuscitation. The automatic external defibrillator(AED) was a real breakthrough. Still, complete recovery eveN in “in-hospital cardiac arrest” is at best 10-15 % . (Brindley PG, CMAJ. 2002. )Here is a technology in-progress story, now I understand FDA has approved this device for emergency resuscitation in cardiac arrest.
The principle is simple. In the early minutes following cardiac arrest, it is the survival of the myocardium and brain that matters. So, occluding Aorta transiently and continuing CPR infuses more life into the brain and heart, and the possibility of revival they say is significantly increased.
Mind you, this is not for the layperson or public but can become a game-changer for the ER crew and in ambulances or even in the cath lab. Emergency insertion of ECMO is never easy and a Neurescue balloon may come in handy in the meantime.
The attraction is the simplicity of the device, just inserted through the femoral artery. Don’t know how successful we would be, in centering the collapsed femoral artery though. The balloon actually doesn’t really impede the lower limb flow.It senses and relaxes as and when necessary.
Final message
The concept behind neurescue looks like a bedside emergency partial IABP-like (IABO-Intra aortic balloon occluder rather) but appears promising. What I understood grossly is, that potential extremity Ischemia is acceptable if it’s going to save a life! Also realize, it is not a magic device that brings back life in every cardiac arrest. It gives us more time to act so that we can do other measures to bring back circulation.
Medical science has evolved over 2000 years and moved far away, from the spiritual cure times at the temple of health at Kos islands to the Imaginations of Davicini. We are now in an era, where we can, not-only take stunning live photographs of individual organs but also go inside, assisted by X RAYs, Ultrasound, CT MRI, and Optical fiber. Now, a new kid is entering ie Holography. (We may expect haptics very soon).
How about a cardiologist operating with a virtual 3D beating heart hanging in front of him?
Yes, it is possible in a scientific fiction movie . No. it’s real. True view, an innovative medical Imaging company from Israel doesn’t think it is a fiction story. The immediate clinical use comes in electrophysiology labs
Breaking new frontiers in medicine is becoming the norm, especially in digital imaging. No doubt, we have entered a new medical world. However, we should be able to realize, that all the excitement is justified, if and only it makes a positive impact on humankind. Even as we are deeply immersed in medical technology, let us remind ourselves, how a tiny virus is teaching all of us, some hard lessons in basic principles and practice of medicine.
Bifurcation PCI is a modern-day Cardiologist’s fascinating professional adventure within coronary arteries. Of course, one of their Intentions is to do good for the patient. Bifurcation lesions (BFL) are a special subset of lesions, that looks challenging, more because of the potential biological aftermath following the delicate construction of a grade separator at a critical site. Mind you, it’s done within a live flowing artery and subsequently needs lifelong maintenance.
Strategies for BFL
Strictly committed* single stent strategy (Irrespective of what may come, LCX or LAD pinching let me take care . Don’t worry strategy *May sound dangerous, but still, it doesn’t make other strategies less ominous)
Provisional single stent strategy with elective cross-over for truly poor result /cosmetic/peer satisfaction purpose
Provisional single stent with bail-out cross-over. Often happen as an emergency (Not all techniques are amenable for this)
Elective planned two stents (Still, flexible to revert to single stent if the situation allows)
Elective, strictly committed, prefixed two-stent strategy (No going back strategy/ Not really a professional PCI )
Always remember, SYNTAX or no SYNTAX CABG is the safe & best bet for many severely symptomatic patients, with complex as well as non-complex BFL lesions esp in diabetic patients.
Wait, there are two more.
7. Please note, there is one benign strategy, that is always available, but hiding deep in the interventional cardiologist’s sub(non)conscious minds. It is a zero radiation, zero contrast, and almost zero cost strategy. Yes, It is “No stent strategy’ also called exclusive medical management, currently referred to as OMT/GDMT. In our analysis of symptom- lesions significance at least 30% of BFL are eligible for exclusive medical management.(FFR & IFRs ? Less we say about it, is better!)
8. One more option for those patients (&cardiologists) who wants to travel the middle path is POBA or a Glorified POBA ie DEB (Ref Corballis NH,. PLoS One. 2021)
Whatever the treatment, bifurcation PCI cannot be taken lightly. One exclusive club is debating this topic in Europe every year (EBC)for the past 10 years. Currently, Double kiss and crush (DK crush) is considered superior to others. Mini crush and Culotte are good alternatives in specific circumstances (Definition 2, NORDIC, BBC 2)
In DK crush every step appears to be double. Apart from the double stent, it is a double wire cross, double crush, double kiss, and double POT (or even more). All must happen in a specific sequence. One may add double Imaging (Pre and Post PCI IVUS or OCT) to the list. Finally and funnily not to miss the realistic possibility of double complications over the provisional strategy.
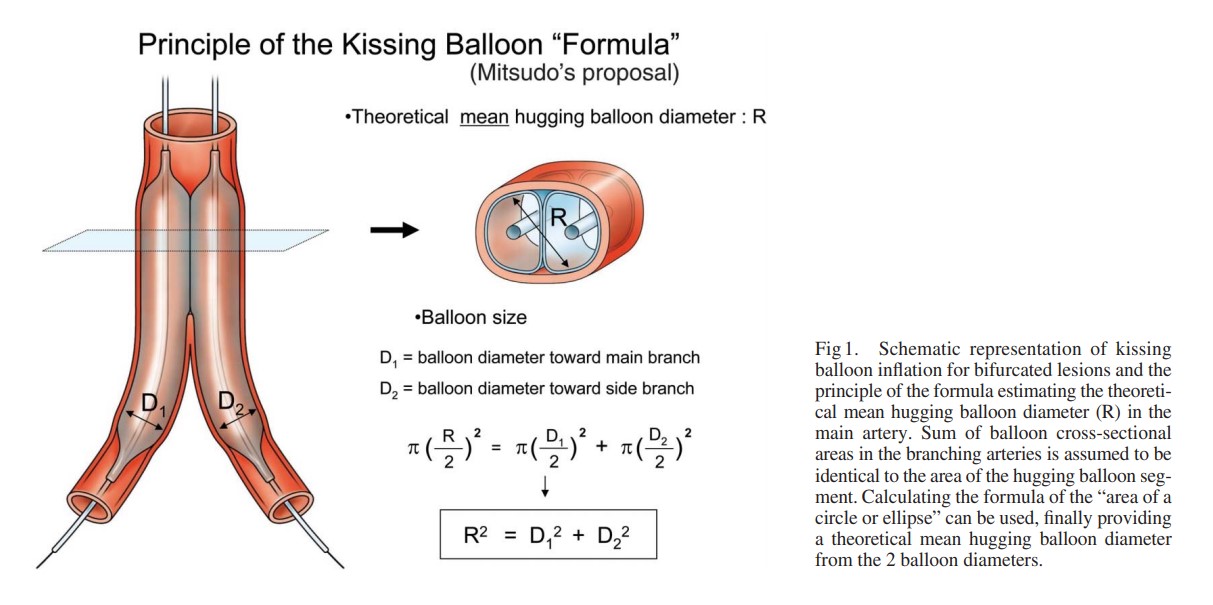
I am not sure which of the 10 steps in DK crush is most important. When we go through the physics of BFL intervention it appears, that proper crushing and kissing may be the key to success. Though kissing is an integral part of any two stent strategies, in DK crush it happens in a unique interface between balloons /balloons with a stent and finally between two stents. In fact
The physics of bifurcation kissing includes balloon hugging diameter, area, and pressure. Added to that is the intervening metal layer.
Can’t take the kissing in a casual manner. The Morino & Mitsuda model tells us more about the physics of kissing. In BFL interventions, kissing can happen with various layers that include one layer of the balloon with a crushed and non-crushed stent, carina. While we are mastering the techniques, we must realize, Kissing is aimed at stabilizing the carinal basement, still, there is a distinct possibility, that what may appear as innocuous kissing may undo all the good work we have done in previous steps. I guess, no harm in missing the final kissing if everything is ok in OCT.
Dr. Anonio Colombo’s take on kissing
Final message
So, we have both simple and complex modalities for BFL. Evidence and experience reveal that 90 -95 % of patients with BFL would be eligible for the easy path. In one sense, we are indeed wasting our energy and resources in tackling this negligible CAD burden located at the summit of the global CAD pyramid with a gigantic base. However, we can feel scientifically happy, that we have gained considerable expertise in tackling complex lesions with multiple stent strategies in recent times. Still, we are far away from a true vision, of what really might follow such a niche & expertise-intensive procedure.
Let us hope, that modern metallurgy in combination with physics & hydrology would ultimately beat Biology.
Looking at the whole issue of complex PCI philosophically, no technique may really be superior based on accrued evidence. In fact, when expertise becomes the key determinant, the evidence goes to the background. It is really surprising we are too much dependent on hasty and often biased evidence to ratify our expertise, technique, or hardware. I know, one of my colleagues can cross any lesion with one or 2 wires.
To insist, that a particular technique must be followed may not be academically correct always. It is similar to telling a coach driver in advance when to apply a brake or accelerator when he is negotiating multiple hairpin bends in hilly terrain on a rainy day, based on clinical trials done with different drivers on different routes. Ultimately, the outcome is decided by the expertise of the driver, the condition of the vehicle, the road, and not least, the destiny of the passenger.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.