“If we are not able to regulate science …what is the purpose of magnificent Inventions & Innovations?”
“Who will take the responsibility for all motivated false research and resultant adversaries?
Final message
Is shutting down (or grossly down-regulating ) research an option?
Foolish option…but
Who Initiated, funded, and masterminded the gain in function experiment with the innocent RNA viruses which were happily enjoying their nucleic acid life, along with the friendly bats in the wild forests, far away from human infestation?
Who ordered to hijack them to (in)human labs and hurt the sleeping viruses with sharp molecular knives to earn its violent wrath?
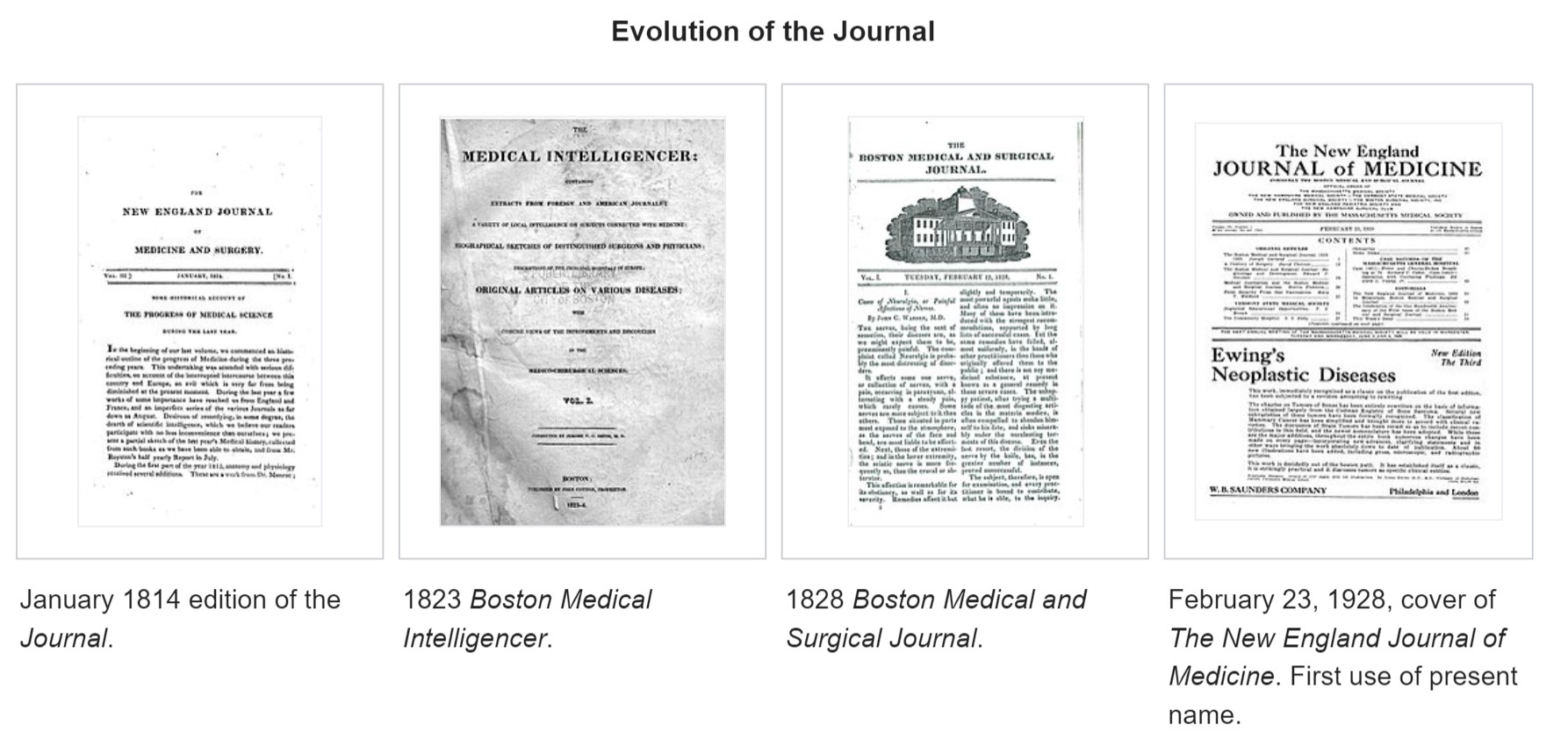
The New England Journal of Medicine (NEJM) the premier journal in medicine originated two centuries ago, in 1811, when John Collins Warren, a Boston physician, along with James Jackson, submitted a formal prospectus to establish the New England Journal of Medicine and Surgery and Collateral Branches of Science as a medical and philosophical journal.
Subsequently, the Massachusetts Medical Society (MMS) purchased the Journal for US$1 and, in 1928, renamed it to The New England Journal of Medicine.
NEJM’s New Journey
It is 2022, after 200 years of providing explosive knowledge in medical science, MMS starts a new journal, fresh and bold. It is called NEJM Evidence. Can you guess, what is the need for such a journal now? I think the most battered word in science in current times is probably “ evidence”. It has a unique character of appearing most sacred as well as scandalous at the same time.
NEJM has remained the torchbearer of almost all advances in the medical field seen in the last two centuries. It is heartening to note the newborn is named as NEJM evidence. It has come at a critical juncture. I am sure, everyone will acknowledge that we are at difficult crossroads. Overwhelmed with unregulated scientific discoveries and publications, struggling to deal with self-inflicted knowledge pandemic. In the process, we have lost “not only” the ability to ignore trivial health issues “but also” failed to provide simple, cost-effective care to the real patients who desperately need it.
Let us hope, (& wish,) NEJM’s new prodigy will guide medical science towards a successful, meaningful, and ethically fulfilling journey for mankind. Meanwhile, let us pray for every medical scientist to be blessed with the required strength and courage to steer in the right direction, weeding off both academic and non-academic contaminants.
What is in store for the future of cardiology as of 2022?
Here is one of the rare lectures (A grand rounds by Houston Methodist) by legendary cardiologist Dr. Euegne Braunwald who shares his wisdom, vision, and research and finally his advice for the generation next cardiologist.
For those, who are short of time to listen to the father of modern-day cardiology, let me share a preview. The talk is divided into 6 subsets.
Polygenic risk score (PRS) Dr. Braunwald talks about how genetic risk profiling and risk factor interaction will help us identify susceptible populations. Here, he stresses also the importance of clinical risk assessment.
Primordial prevention of CAD:
Anti-lipid strategies:
He introduces a new concept of Cumulative LDL score & CHD threshold. Dr. Braunwald argues rigorous lipid control should go beyond statins and suggest once a year Injection Inclisiran(Small interfering RNA that prevents PCSK synthesis) will reset the lipids levels by 40% and prolong life by 30 years.
Anti -Inflammatory strategies: He reminds us Atherosclerosis is equally an inflammatory disease and new anti-inflammatory drugs like Canakinumab’s role could be vital.
Artificial Intelligence: Will be the guiding force in the future of preventive cardiology, as well as treatment. He tells us predicting Atrial fibrillation and even LV function from the resting ECG is possible.
Clonal hematopoiesis independent potential (CHIP) is a new risk factor by somatic mutations in leukocytes that accelerate atherosclerosis proven by canonical risk predicting models
It was a great one hour to spend on a Sunday, under Covid Lockdown. However, It was a surprise, the biggest Innovation in cardiology in the last century, PCI, and other exotic coronary and noncoronary interventions could not find a place in his one-hour lecture. I think there is a hidden message here.
He signs off with some important advice for the generation next cardiologist.
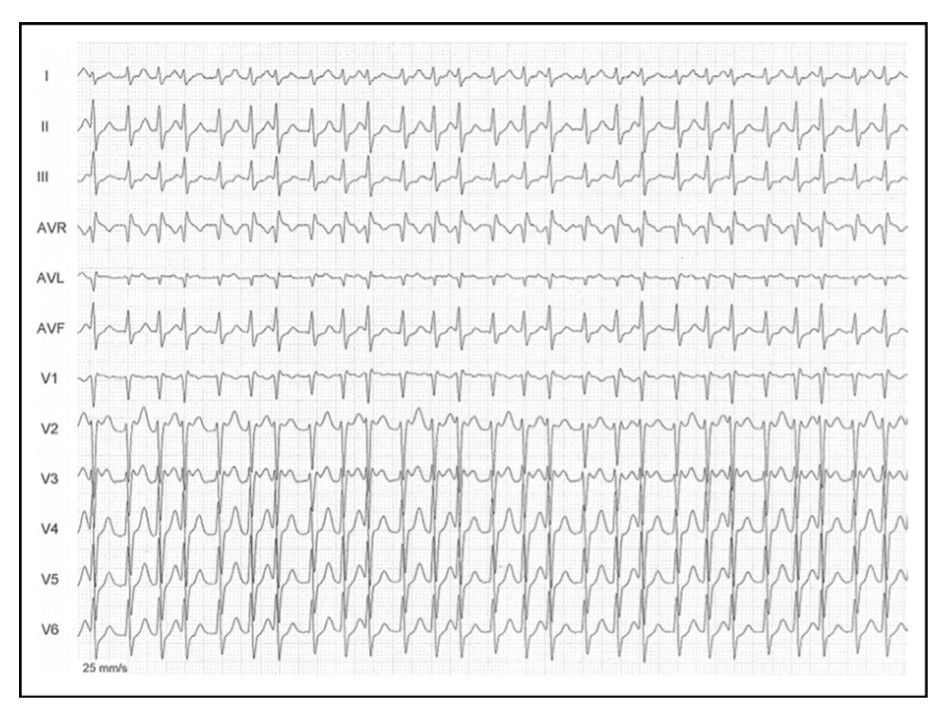
Here is a case report from Dr. Brugada’s group. What is your diagnosis?
Source & Courtesy Sergio Richter, Joseph Brugada et all , 100(1), 154–156. doi:10.1016/j.amjcard.2007.02.067
Whoever diagnosed AF in the above ECG need not feel bad. The rhythm is not AF, though it mimics very closely. In cardiology, especially in electrophysiology, we can get surprises on a daily basis. (Read below)
Why the ventricular rate is irregular in AF?
Atrial fibrillation (AF) may sound like a simple clinical arrhythmia until we ask this delicate question. The traditional and fairly accepted answer is that, AV node with all its collective decremental property filters the incoming atrial impulses (Which varies 400-600/mt) in a random fashion and allows only about 1/3rd of impulses. So, technically it is AV block of various degrees that makes the ventricular response irregular.
Any other explanation possible?
How about AV node playing out a silent game with Atria, deciding to block everything and start its own fast escape rhythm, rather than leaking out selectively atrial impulses. Some think this is fictional, some others feel it can be real too. When this happens it can be referred to as irregular junctional tachycardia or AF with varying AV blocks. It has been tough, to prove it is only the atrial impulses penetrating through the AV node complex and exiting on the ventricular side unscathed?
Understanding AV node is not easy
AV node morphology and function still remain a mystery.( Katritsis DG. Arrhythm Electrophysiol Rev. 2020)The AV node shows huge variation in its size, shape, orientation with LV long axis and AV plane in short axis. The approach to slow pathways with multiple inferior nodal extensions makes a dual (or even poly ) AV pathway in any human being real. How common is dualism or multilateralism within the AV node in the general population? (More than 30-40 % ?) . Let us also mind the traffic in this busy & complex AV flyover can change on a moment-to-moment basis based on neurohormonal and autonomic tone.
Any tachycardia can become irregular if the AV node wishes so !
Though rare ,multiple physiological splits in the AV node make it possible for a single atrial impulse can generate 2 or 3, even more, ventricular impulses. (1: 2 or 3 AV conduction) Since these pathways are dynamic they can make the ventricular response irregular as well (Unlike the regularly coupled Echo beats in classical AVNRT substrate ). Hence, any supraventricular tachycardia can masquerade as AF if AV nodal pathways decide to split and share the impulses this way. It is also interesting to note there has been a documented link between AVNRT and AF (.Ref 2) . Also, adenosine-induced AF is known (James E. Ip et al Circulation: Arrhythmia and Electrophysiology. 2013;6:e34–e37)
Final message
Irregular RR interval with absent/or invisible P waves is not always AF. It can be due to the aberrant behavior of the AV node.( anatomical or functional) It is termed Pseudo Atrial fibrillation as in the above case report. Why do we need to be aware of this entity? We need to be cautious, as any overzealous efforts to ablate the pulmonary veins in such patients will go in vain.
A 5-minute session: Answers are my own. Please cross-check.
1. Is Brugada syndrome clinical or ECG diagnosis?
Always clinical. Never get confused on this.
2. Spontaneous type 1 vs Induced Type 1 (from type 2) which carries more risk?
Both are risky since they are close cousins. But, spontaneous type 1 is the dreaded devil.
3. Is Brugada primarily a defect of myocardial depolarization or repolarisation?
Not clear. Often in both. In fact a mismatch between them. (Don’t ask how Na+ Channel defect affects repolarisation !)
4. Is Brugada VT is monomorphic, polymorphic?
Both. What determines morphology is not clear though. (All de-nova monomorphic VT will degenerate to polymorphic en route to cardiac arrest)
5. Should Fever induced Brugada pattern be investigated further?
Better, it is not to be reported in ECG. May not be important in the majority if there is no adverse family history. (If the patient is well educated and afflicted by Dr.Google and cardiologists can’t escape from ordering sophisticated tests)
6. What is the overlap between ERS and Brugada?
It is all about the Idiosyncrasy of the K+ channel phenotypes ( Transmural dispersion heterogeneity )
7. Is a benign Brugada better than a malignant ERS?
Yes, it would seem so. (Inferior or Infero -lateral ERS prone for primary VF in case they develop ischemic / ? also non-ischemic stress)
8. How important is the link between Brugada and Long QT 3 syndrome?
A rare entity, but It is double jeopardy for VT risk. The entire action potential width is vulnerable right from phase 0 to 3 or 4 A case report Sandhu A Clin Case Rep. 2017;5(8):1315-1319.
9. Is Amiodarone really contraindicated in VT?
Not really. Though Amiodarone unmasks Brugada, it can still be used during episodes of VT in patients with manifest or unmanifest Brugada. Maybe in Long QT 3 overlap, it may perpetuate the VT.
10. How important is the structural myocardial defect in Brugada?
Not important in the majority. Though localized RVOT abnormalities are noted in some..RV abaltion can be succesful in odd case.
11. What happens to the ST segment in Brugada during exercise stress?
Obviously not. But, definitely life-saving in high-risk survivors. I guess definitive therapy is possible for future generations through the science of genetic reprogramming of Na+ channels. (Of course, our planet shouldn’t succumb to man-made climatic arrhythmia, by then )
14. Does widespread genetic testing & screening of families help in the management and reduce anxiety?
Cracking the genomic code of cardiac ion channels is the ultimate sophistication (Blueprint of fate ?) However, there is no guarantee this information is going to ease out the family members who harbor a genocopy with or without a phenocopy.
15. Is Brugada getting undue attention in cardiology literature compared to many other common arrhythmias?
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.