“Never take your eyes off the monitor and the pressure curve” It is one of the basic instructions given to the fellows & technicians as they start engaging the coronary artery and Intubating the coronary ostium in their early cath lab postings. There are two commonly heard noise bites in the cath lab for the beginner. 1. Damping 2.Ventricularization.
Damping
It is the deformation of the normal arterial pressure curve, with a blunting of both systolic and diastolic pressure that drops compared to aortic pressure. Extreme damping can mimic a straight line with few wavy undulations. It means the forward flow is impeded as the catheter might be blocking the coronary flow at least partially, if not completely. Immediate pull back and adjustment of catheter is required to prevent adverse events that includes cardiac arrest. (Of course, catheter kinks, blocks, and air in a circuit are to be ruled out first)
Mechanism of damping
- The catheter tip is too large for the ostium.(Technical)
- A left main or RCA ostial lesion*(Most significant clinically)
- The coronary artery wall is thin and goes for spasm
- Catheter diameter is too small and glides into the coronary artery (The catheter tip hitches against the lateral wall of the coronary artery often over a plaque, a silently staged perfect setting for a dissection )
Unique features in RCA damping
In RCA, damping could simply mean it has engaged conus branch. Damping is more common in RCA and it tends to get sucked in deeper for two reasons. We know , the RCA catheter is not preformed, the tip seeks the ostium, looking for a negative pulling pressure from within the RCA. Further, unlike the LCA, the flow in RCA is continuous in both systole and diastole. Another possible factor is the inspiratory swings of RV transmural pressure is more than LV.
Transient bradycardia due to compromise of SA /AV nodal flow is common. It is well known that RVOT is a thin and VPD-prone zone , compared toLVOT. Hence it is more vulnerable to ischemia and triggers a VT/VF if damping is prolonged in RCA.
Ventricularization

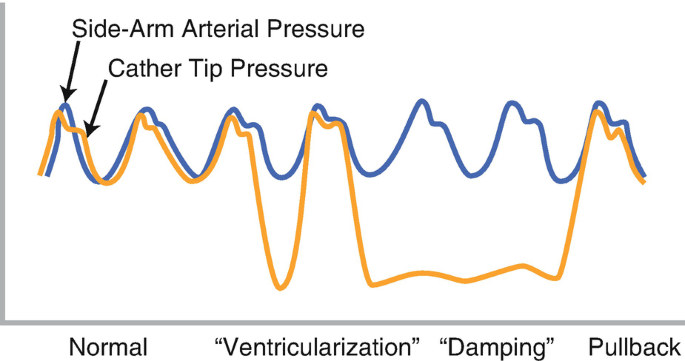
This is tracing during the engaging of a left main ostial stenosis. The diastolic pressure drops on the third complex, and the pulse pressure becomes large . Note the small “a ” wave slur as well near the diastolic nadir. The aortic pressure curve is restored once tip adjustment is done. Image courtesy Thoraci key.https://thoracickey.com/coronary-angiography-3/
It simply means the pressure curve starts looking like a ventricular pressure curve. The issue is not that simple. It is still a mystery, how could the coronary artery pick up ventricular pressure. In fact, it doesn’t. It was initially thought to be either deformed aortic pressure or a wedged coronary artery pressure .or a combination of the two.
It s now accepted it’s due to total occlusion of the coronary artery the ventricle muscle sucks the catheter and pulls the diastolic pressure markedly down even lower than LVEDP. The systolic pressure also falls but not much of it is noticed.The fact that ventriculaization happens less commonly with RCA gave us a clue to its mechanism. (Most of the RCA travels over RV and since RV muscle mass wields less negative suction force )
How to differentiate true LV location from ventricularization?
If the catheter enters the LV cavity, the systolic pressure will match that of aortic systolic pressure and diastole will reach the LVEDP. In ventricularization there can be a slight drop of the systolic pressure, but the diastolic is the one goes far down. Further, the ascending limb is shallower, the descending limb is steeper in coronary ventricularization. Apart from this if we carefully look “a” waves will be visible in ventricularisation in the late diastolic phase.(Could it be the modified Incisura ?)
Relationship between damping and ventricularization ?
Discussing damping and ventricularization together is more of an academic tradition. Please realize, both may not be two exclusive entities. In fact, they can occur at the same time, or sequentially or interchangeably if the catheter tip swings back to partial to total occlusion and vice versa. if complete wedging occurs it becomes ventriculariszation.
Which is more dangerous damping or ventricularization?
How can you ask such a question? Both can be harbingers of serious hemodynamic issues if ignored and accidentally injected, The dreaded one is the dissection. Apart from mechanical injury, Injecting dye during damping or ventricularization causes dye stasis, and may trigger VT or VF if it is prolonged. There is a biochemical component too. As the contrast swirls around for a few seconds it can cause transient hypocalcemia by chelating this cation.
I don’t have a clear answer to the above query. In my understanding, forceful injections during ventricularization could be more riskier as injection happens over a total occlusion in a wedged position and dye has direct access to the microcirculatory bed. It is true, expert cardiologists do shoot in damped positions occasionally to see the anatomy quickly. They may be your mentors, still don’t learn this trick, till you become a true expert (Famously referred to as hit and run technique)
How to overcome these pressure curve malformations?
Most times, it is a simple technical artifact issue. Deep Intubation with an oversized catheter could be the commonest cause in the otherwise normal coronary artery. Proper catheter sizing, angle of alignment, and adjustment is the key. If it is a spasm nitroglycerine might help. Using catheters with side-hole perfusion catheters is an option in difficult anatomies. Mind you, side holed guide is a two-edged weapon, it can mask true hemodynamic adversaries by falsely showing a good aortic pressure tracing.
(One of the good cath lab habits is to have a look around the patient face at least once in a while when performing complex procedures. We have many times recognized serious hemodynamic issues only after the patient starts behaving bizarrely due to hypotension. Pressure curves can fool you, but patience will never.)
Final message
Recognizing abnormal waveforms during engagement is a crucial step for the beginner (Experts can’t ignore though) Please remember LMCA stenosis should be the default alarm for any damped pressure curve as you engage the LCA. If you take things casually consequences can be lethal for the patient as well as the consultant in charge.(Fellows can’t take it lighter though). It is an undisclosed fact, that many of the serious complications in the cath lab happen not out of ignorance or lack of expertise, but because of ignoring some basic principles and lack of cath lab discipline.
Reference
1.Baim DS, ed. Grossman’s Cardiac Catheterization, Angiography, and Intervention. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006. 2. Judkins MP. Selective coronary arteriography, a percutaneous transfemoral technique. Radiology 1967;89:815.
2.T Pacold I, Hwang MH, Piao ZE, . The mechanism and significance of ventricularization of intracoronary pressure during coronary angiography.Am Heart J. 1989 Dec;118(6):1160-