Any structure which has a foundation on which it stands is generally called base or basement. By tradition base is synonymous with bottom .Ironically , for heart this rule does not apply. This is the core area of confusion. The heart is a complex shaped 3D organ with multiple surfaces with 4 chambers connected each connected to its own great vessel .
We know heart is simply suspended by these vessels inside the middle mediastinum and anchored with ligamentous attachment to chest wall, diaphragm through pericardium .
Now, traditionally the heart was thought to be cone like stricture with apex located near the left mid clavicular line .
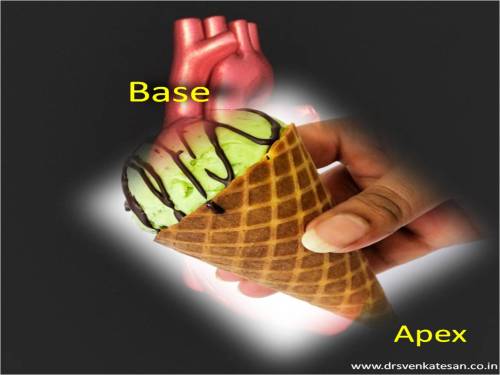
If there is an apex there must be a base .So , we reasoned the highest and farthest part of the heart must be the base . Paradoxically , this base is at the top , and not in the traditional sense of bottom .
Like wise , during auscultation the events in the base represent the great vessel and semilunar activity (Anteriorly )
Baseless base
Clinical base is not the anatomical base . When a patient lies on his back essentially the atria and posterior aspect of ventricles form the base . In erect posture the diaphragmatic surface becomes the true anatomical base of the heart .
Further confusion during Echocardiography
It is well known , basal LV function is a critical determinant of LV function .But we should be very clear what area we are talking about ! Basal aspect can lie either superior , inferior , anterior even posterior surface of left ventricle .(It took me years to realise this simple fact !)
Similarly basal septum can mean either a LAD zone or even RCA zone one has to specify basal anterior septum to define LAD zone ischemia .
(Please note , this is contrast to clinical cardiology where the base of the heart refers only to anterior aspect of heart ! )
FInal message
Calling a particular portion of the heart as base would be an anatomical misnomer . This nomenclature is based , more by tradition and our faulty perception .(As visualized by anatomists and pathologists )
We have come a long way from the Da Vinci days. Modern cardiologists with sophisticated imaging techniques would like to call the basement of heart differently in the future and correct the nomenclature issues.
Read Full Post »