We know, The Mysterious Alibaba cave opens with a voice password . . . legend tell us it had unlimited hidden treasures. It would appear , CTOs mimic the cave in several ways. What is inside ? Should we open it ? Can we come out safely ? Do we have any magical password in cath lab to get across the complex tissue boulders ?, every cardiologist would love to have one !
Dear CTO,Open Sesame . . . I have come with all the wires you love ! Please let me in !
Indication
“CTOs are never an emergency . . .but please realise we can very easily create one while resuscitating a dead snake !
Don’t think hard on evidence , then , you may not do a single case of CTO in your life .Forget all those pessimistic trials like OAT,COAT, etc and the recent ones DECISION-CTO. Ignore all guidelines. Ask your patient, and his insurance company , if they are willing , reserve the cath lab and get ready.
Pre-procedure planning
Spend at least a hour to analyse the CTO Imagery one day prior and create n action plan.
Keep knowledgeable staff for assisting , but never ask for fellow colleagues help because it hurts our ego ! Cardiac surgeon’s back up is a welcome addition even if it’s on paper.
If possible , try to ask the patient genuinely ,what is his symptom at least once ! before starting the procedure.
Timing of the procedure.
Don’t post a CTO patient either on a busy Monday morning or lazy Friday afternoon.
Hardware Inventory
The wires ,catheters, the balloons form the essential tool box .There is more than a handful of coronary automobile companies manufacture this .It is all about metallurgy , knowledge of wires, catheters , and tip thickness, (Bullet shaped as in Asahi ) , slipping , hydrophophic or philic, polymer coating , trackability, pushability , memory etc etc.
Guide wire tip morphology is as Important as the Lesion characteristics !
Analysis of the lesion (Probably most important)
Unlike conventional PCI we have no initial target.We need to poke first and find the target next ! Distal vessel status is most important ( Careful review of retrograde filling through collaterals could give more information than CT angiograms .Calcification, diffuse disease can be a real hurdle)
Lesion morphology
Softness of lesion has to be felt (Requires good wire which has sensor (Paccinian corpuscles and Merckle disc ideal ?) I guess the cortical tactile feel is as vital as the intervention expertise .I know at least one diabetic colleague of mine who finds it difficult to cross a CTO and admits he never found it easy to feel the lesion through the wires . Autonomic dysfunction ?)
Operator expertise
(Note: These are like reading swimming guidelines , you can’t learn in the shores reading books ! you have to plunge !)
Many techniques are proposed .Sequential approach (Ironically experts are licensed to use specialized wired wires directly .Beginners are advised to go with non specialized hardware and escalate step by step) Some centers are blessed with new age weapons like cross Boss and sting ray that confront the lesions in multiple frontiers. (Carpet bombing?)

CTO playground. : Its essentially a coronary contact sport with expert septal surfing , tunnelling, knuckling , kneeling , bending . Of course , It can end up in a gratifying win in few , still most of us tend to play this game without a goal (post !) Source of the Image : Unknown Due credits to the creator.
They are basically about poking the head of the lesion and trying to cross an occluded vessel millimeter by mm towards the presumed distal vessel in an Imaginary trajectory. Proximal cap, central core ,the blind tunnel , distal capsule and exit points each must be successfully conquered.
CTO crossing is the ultimate capacity of the operator to realise and feel the position of the wires in true lumen and their confidence levels in their conviction!
Multiple wires up to three are used some times to poke the lesion two of them are used to shut the false tracks and the other one is expected to enter the true lumen (Looks too good on theory !) . These are referred to in as many terms like parallel wire see-saw , CART ,Reverse CART etc .Retrograde techniques do help us but has no magic solutions.The lumen contrast , guide wire tip movement and its side branch entry would help.
Tacking complication :Always anticipate , it’s not negative mind set to look for it !
Keep pericardiocentesis kit , covered stents , micro snares and other retrieval devices ready in cart. Your support staff should be well versed with what is happening around them. Some of the dye leaks and stains are safe .They imply minor perforations that form sealed hematomas (The plane of perforations also matters. myocardial (ab-pericardial ) leaks are well tolerated .Distal perforations are also safe as long as CTO is not opened ) Online echocardiography should be readily available to monitor pericardial space leak.
When bleed into pericardial space is life threatening , A comical, but life saving option is to close the artery and restore the CTO its original state and come out of the lab quietly !
Newer Imaging guidance : Can be useful , still may not matter much when considering the interventional acumen .
CTO PCI : Time as therapeutic end point.
CTO is not an endless game with out time frame .In my opinion it shouldn’t cross 45 minutes each as in a soccer game with a brief strategic time out and of course with liberal use of ,yellow and red cards
Future directions
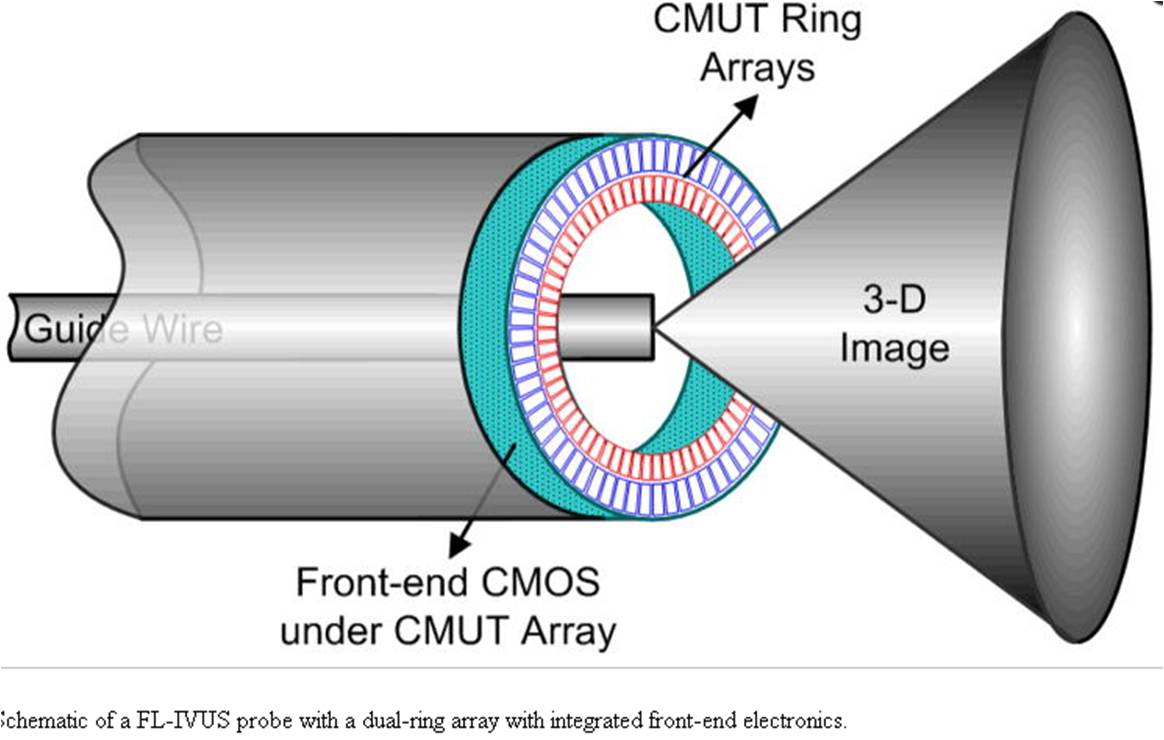
Japanese are the ones who pioneered CTO Interventions . We expect more Innovations ! Is it the forward looking IVUS ? It is akin to tunneling for underground metro train with GPS guiding .If you can mark the proximal and distal points , rest will be be taken care by mortised self tunneling catheters from Robotic arms steered by sophisticated algorithms.
Final message
CTO PCI remains a real Interventional challenge. We are often double blinded in both directions (antegrade as well as retrograde ). Needs much effort ,time, hardware and most importantly a non fatigued mind and body. The benefits we get may vary between gratifying to outright mediocre .Of course , it surely satisfies operator ego and express pride and courage !
Is crossing and stenting a CTO synonymous with true success ?
Yes it is , for the cardiologist and the hospital . . . I’m not sure about it for the patient !
In this sense , CTOs mimic the mysterious Alibaba cave that tempts us with Imaginary treasures but can trap us with a wrong password !
Post-Ample
* Who should CTO PCI ?
I have seen young , enthusiastic cardiologists with Immature support staff attempting CTO in remote sub- urban settings ! Though patience and expertise are essential ingredients, some amount of organised training and hardwares make CTO PCI safe and effective. Enthusiasm and affordability alone can’t be an Indication for this complex set of coronary lesions.
Reference

I still wonder why this vital paper was never published , it was just presented in the Annual ACC conference March 2017
http://www.eurocto.eu/
http://www.cct.gr.jp/
Read Full Post »









{kind=link}