Aortic stenosis evaluation was simple in our days. Gradients across the valve were the key. Now, we have more parameters to bother about. Dynamic AVOs, flow state, resting LV function, contractile reserves, GLS, dobutamine response, etc. MRI assessment will soon overtake echocardiography.
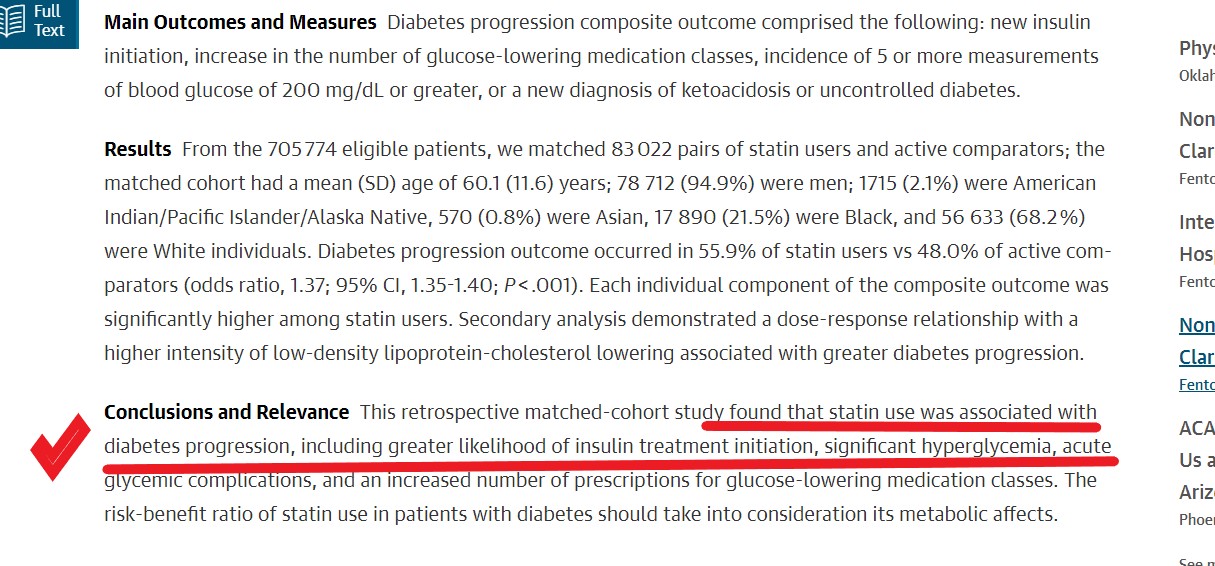
Hemodynamics of flow across LVOT. MRI 4D volumetric model of normal Aortic stenotic flow in the bicuspid valve (On the left). The more we know, the more we tend to miss! Image courtesy: Northwestern Medicine
The current AS algorithms, though scientific, I am afraid, appear much complicated with some frightening terminologies at least for the beginner. One such category is PLF-LG-AG.
Let us first answer this. What is LG-AS?
We diagnose a case of significant aortic stenosis but desperately miss to pick an adequate gradient across the valve. It is indeed a low gradient AS, still, you are not convinced, since the 2D look of the valve looks severe. Then you find the culprit. It is the dysfunctional ventricle pulling down the gradient. This is called LG-AS.(one type )
*What is paradoxical -Low flow-Low gradient Aortic stenosis? (PLF-LG AS)
Now, we have another patient. Again it is LG-AS, but the LV function and EF are normal. Now, you get confused and label it as PLF-LG-AS.
PLF-LG AS is known to account for approximately one-third of patients with severe AS and preserved LV EF.PLF-LG severe AS is defined by AVA <1.0 cm2, indexed AVA <0.6 cm2/m2, mean gradient <40 mmHg, LV EF ≥50%, and low transvalvular flow (indexed stroke volume <35 mL/m2).
What is the paradox?
AS is severe, but the gradient is not showing at the valve. Wait, don’t think that is the paradox, since this can happen in any category of LG-AS. So, the real paradox in PLF-LG-AS denotes to the fact that the gradient is low, in spite of normal LV function (Rather, normal EF %)
Why the paradox? Why gradient is not showing? (In spite of good Ejection fraction ?)
- Reduced stroke volume increased afterload due to associated HT are the major hemodynamic mechanisms of PLF-LG AS.
- The low-flow state can be related to small LV cavity
- Significant diastolic dysfunction (Associated Amyloidosis is a new age problem kid on the block. EF is not the only parameter that can compromise the flow you know !)
- Atrial fibrillation (Ofcourse some cycles will pick up the high gradients, but are they spuriously low or high is the question )
- Associated mitral valve disease leaks, as well as blocks, will ration the flow to LVOT.
*Finally, every cardiologist should be aware of the following two subsets that could wrongly enter this conundrum of PLF-LG-AS without much fanfare but with lots of implications.
1. Most importantly, technical issues are the key confounders. Malaligned LV / LVOT with that of distorted out-of-plane AVO is the commonest cause of failure to pick up the gradient. (Never diagnose PLF-LG-AS without confirming it is not due to technical ). A tip: Don’t complete AS doppler study without a meticulous search for a good doppler signal from the suprasternal/right parasternal window.
2. Next one can be named with a provocative term “Paranoid aortic stenosis*”. Once, a fellow was reporting a shabby-looking calcific valve as low gradient, severe AS with normal LV function. He made this diagnosis solely based on AVO. Later, when it was assessed more scrupulously it turned out to be a true mild aortic stenosis, and none of the decorative echo features he was showing were really pathological. It was an error in the aortic valve area calculation due to LVOT area/VTI measurement errors that got mathematically amplified. An important teaching point emerged from this echo lab fiasco. Mind you, any true mild aortic stenosis (If the area calculation is wrong for some reason) will readily fulfill the criteria of PLF-LG-AS. One simple tip: Never diagnose severe Aortic stenosis without significant LVH.
What is the role of Doubtamine stress echo in PLF-LG-AS ?
It does help in both forms of LG-AS. You need to read about the contractile reserve, the response of dobutamine to flow (Cardiac index), gradient, and the valve area.
How to manage PLF-LG-AS ?
Many of them might be argued to end up in TAVR. So, follow the guidelines carefully but don’t apply them blindly
Final message
In the evaluation of Aortic stenosis let’s make things simple. Gradients are indeed important. But, realize Doppler gives only pressure data. Converting them to flow and volume data is always error-prone. Instead, let us believe our eyes too.(Need not always depend on o MDCT vision) Concentrate more on LV morphology, valve pathology, and careful assessment of LV function, finally take a decision to intervene based on true symptomatology and comorbidity.
Reference
1. For the most authentic knowledge base
2.An excellent review on the topic
Guzzetti Ezequiel Frontiers in Cardiovascular Medicine 2020
Further thoughts
Is there a “high flow-high gradient”- True mild AS?
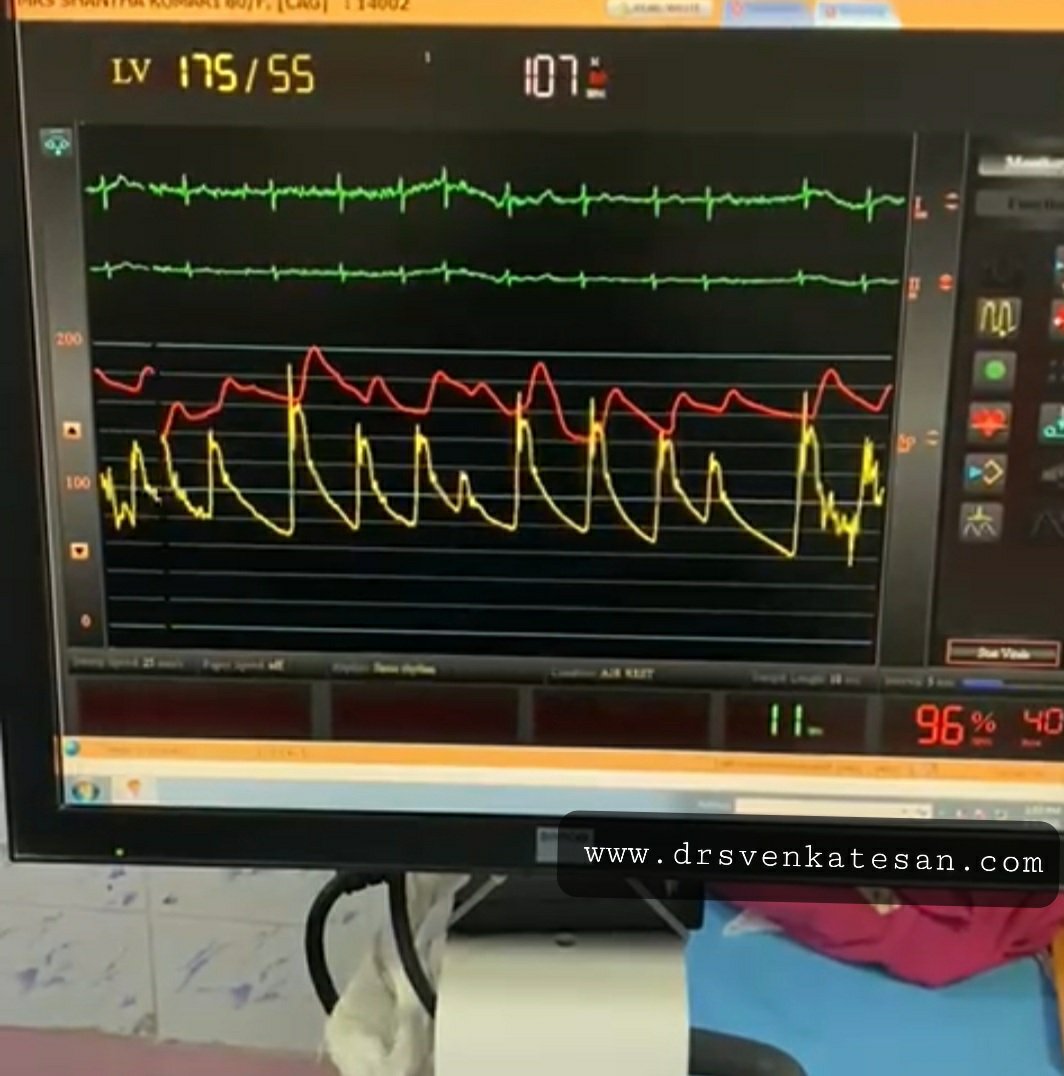
High gradients across the AV generally do not cause much confusion. If the mean gradient is > 40mmhg Aortic stenosis is always severe. Is that right ?. I think so. Exercise-induced paradoxical high flow high gradient AS as an entity is not reported as such. But, what really can happen in high output states, hyper contractile ventricles with high EF? We have observed doppler gradients overestimate the severity of Aortic stenosis. I think there is some dynamic component even in the so-called fixed valvular AS that alters the gradient in response to flow. Do we have proof for this? OMG, it’s right there in echo lab every day, we are failing to notice it. Look at the AS gradients during AF. It is changing every beat, right.
Read Full Post »