
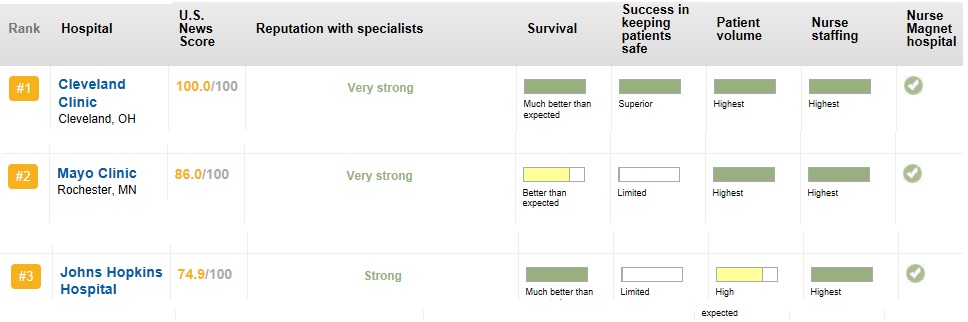
The top 3 cardiac care hospitals for the year 2012-2013
- Cleveland clinic
- Mayo clinic
- Jhons Hopkins Hospital
//
Posted in Top ten in cardiology, tagged America's top hospital, cleavland clinic mayo clinic jhon hopkins, us news and world report top hospital 2012 2013 on May 31, 2013| 1 Comment »
The top 3 cardiac care hospitals for the year 2012-2013
//
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, Cardiology-Arrhythmias, Infrequently asked questions in cardiology (iFAQs), tagged priamry twisting of t waves, repolarisation alternans, T wave alternans, torsades depointes and, twist dance of heart death dance, Twisting of qrs and T waves on May 31, 2013| Leave a Comment »
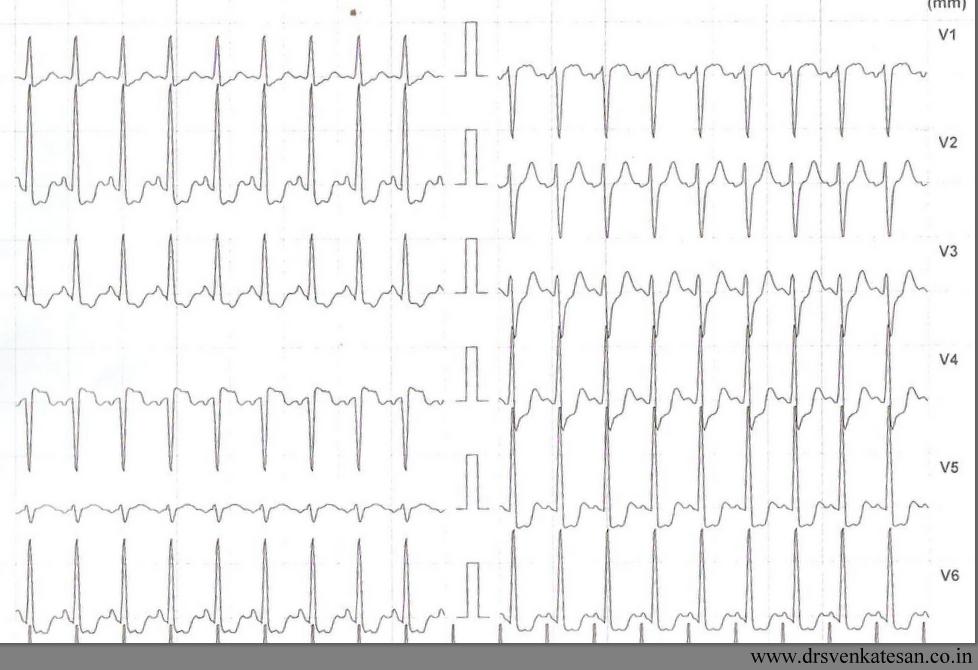
It is believed T wave alternans is a marker of impending ventricular fibrillation. Though it is not applicable in every clinical setting it is indeed true if we observe T wave alternans in an acute ischemic setting .Here is a patient with ACS and inferior MI who developed T wave alternans after temporary pacing.
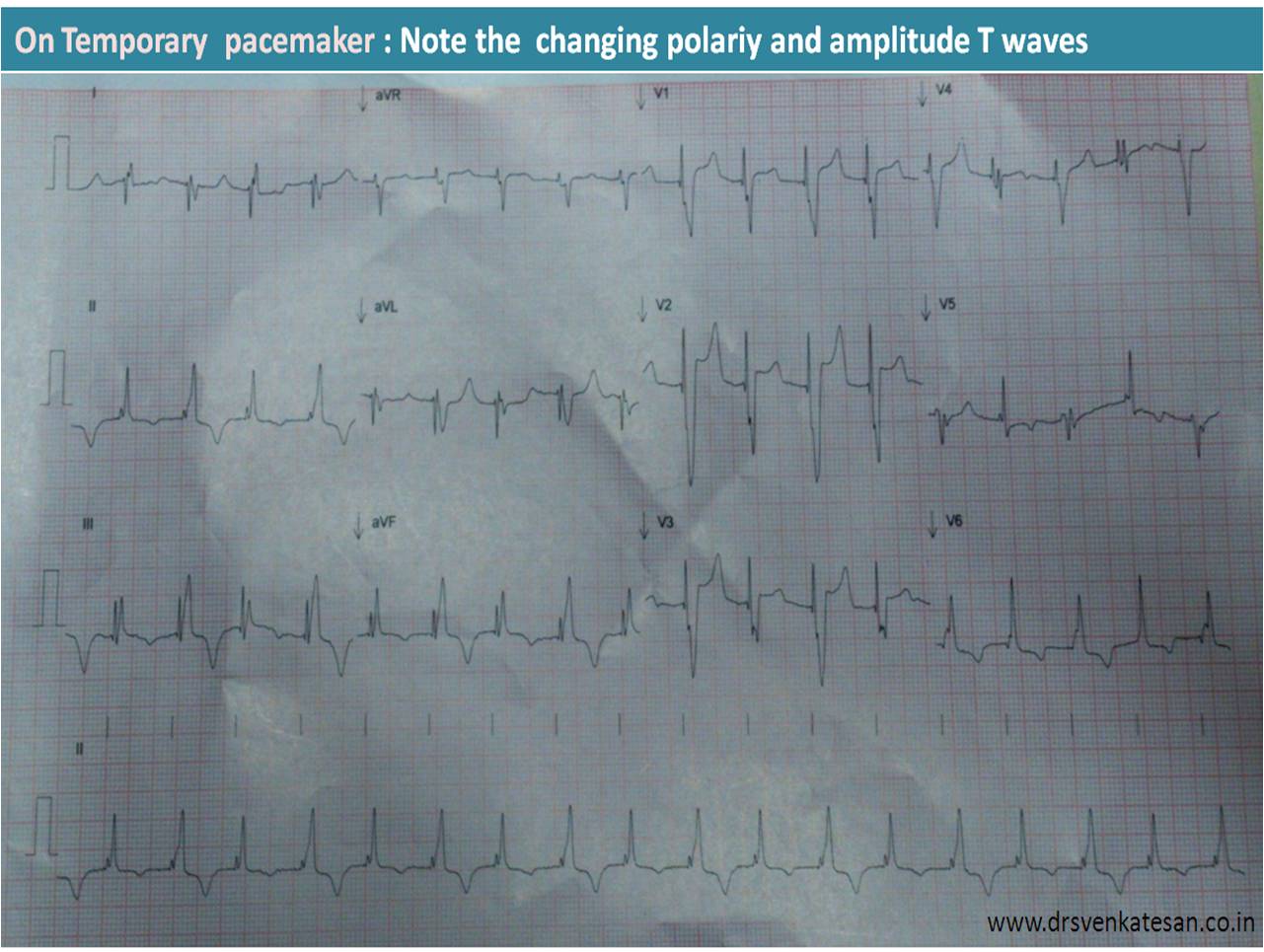
went in for a chaotic T wave rhtythm and ended up in VF that required s shock.T wave alternans is other wise known as repolarisation alternans .
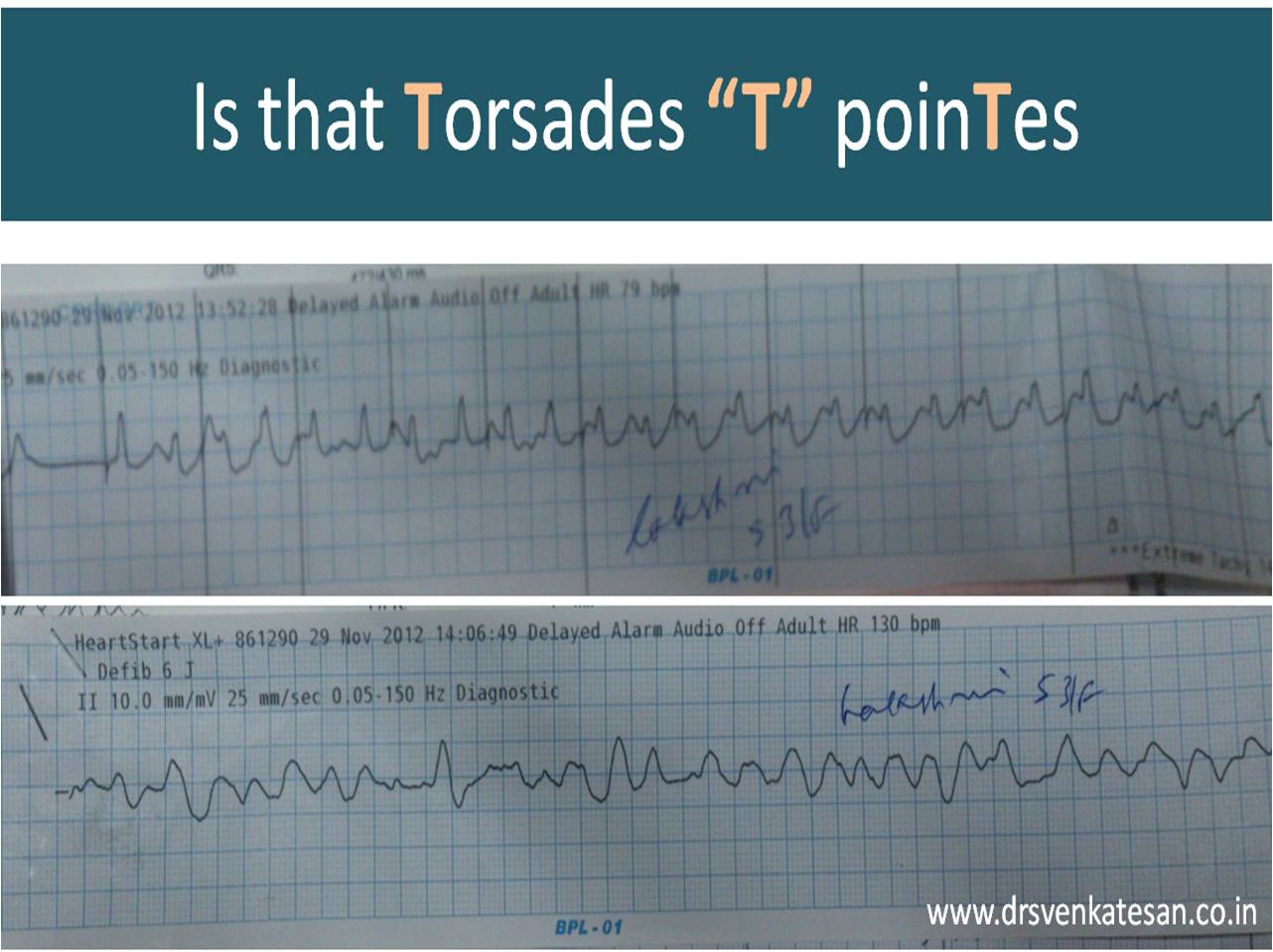
Twist dance of Heart
Torsedes is twist around it’s axis. Any ECG wave can twist in it’s axis .If T wave alternans becomes gross it will twist 180 degrees .Once this happens the heart can go for fibrillation any moment !
Final message
Extreme form of T wave alternans would result in complete twisting of repolarization vector which is a harbinger of ventricular fibrillation
I wish this can be referred to as Torsades “T” pointes instead of Torseades “de” pointes
Posted in Cardiology -Interventional -PCI, My presentations, tagged follow up of pci patients, management of post pci patients, pci ptca, ptca ppt on May 31, 2013| 1 Comment »
Click on the file to download the presentation
Note : The contents are prepared in 2006 .Recent input are to be added .
//
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions, tagged demand ischemia and unstable angina, mechansim of unstable angina, secondary unstable angina, thrombus less unstable angina, unstable angian without thrombus on May 31, 2013| Leave a Comment »
Thrombus laden plaque is sine qua-non of UA/NSTEMI . That’s what we have been taught ! right ? It may be true in many situations , but please remember there is another concept called demand ischemia , where in there is no active thrombus , still resting angina may occur due to increasing heart rate etc.
I just wanted to test how far this concept is understood , by the fellows in our coronary care unit . Following is story of a patient who arrived at CCU with angina at rest . I showed this ECG asked them the management .
History was purposefully blinded . 5/6 cardiologists wanted to admit the patient either in CCU or rush to cath lab. Heparin/ Fondaparuinux was prescribed by all. Tirofiabn was suggested by few.It is a high risk UA with left main disease some one mumbled .
I silently listened to them and revealed the history . This patient has just finished the exercise stress test , it was terminated as he had angina at peak exercise. and was reported as positive . A date was fixed for elective coronary angiogram. 10 minutes later ECG totally normalised , and the patient went home (Boarding a crowded Chennai city bus )
The fellows realised the importance of history . In fact no body asked for it ? I felt bad as all my fellows failed in this test That reflects bad teaching on my part !
What is the mechanism of ST depression here ?
(Severe forms of stable angina can occur at rest . So do not equate all rest angina as true unstable angina !)
Final message
Do not label an ECG straightaway as acute coronary syndrome when there is baseline tachycardia and ST depression . Spare few minutes and apply your mind !
If a combination of ST depression and angina can be taken synonyms with UA every EST positive fellow should be labeled as UA and admitted in CCU. Please remember any tachycardia with a fixed tight lesion will mimic UA . Further , since there is no thrombus here and there is absolutely no role for heparin.
Posted in Cardiology - Clinical, cardiology -ECG, Cardiology -Interventional -PCI, Cardiology -unresolved questions, Cardiology-Coronary artery disese, Clinical cardiology, tagged ECG, how to measure st segment elevation on May 31, 2013| 1 Comment »
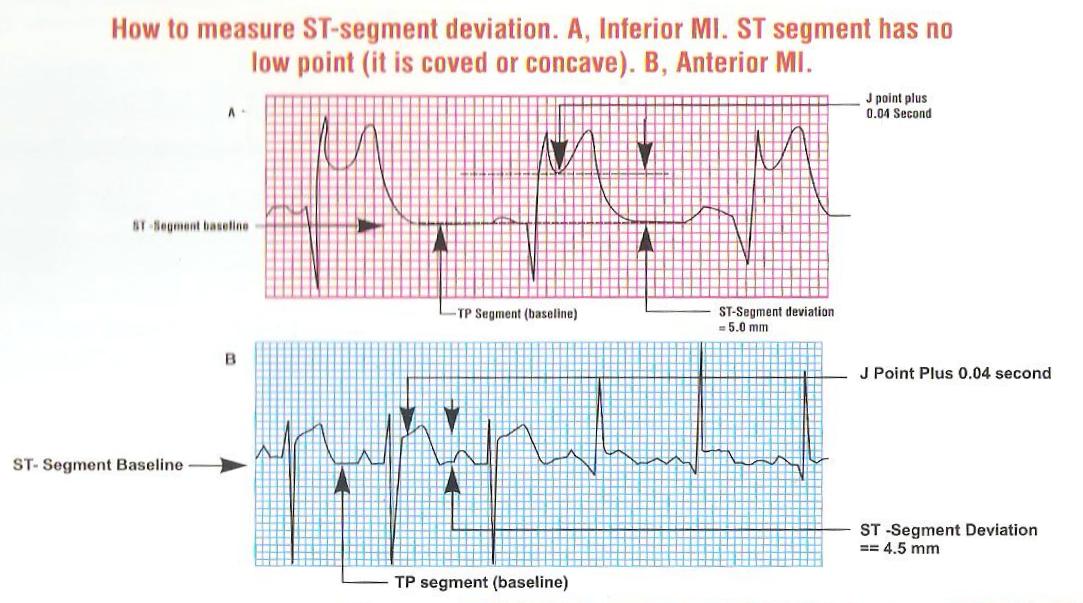
ST segment elevation is the key parameter on which the fate of millions of infarct patients are recognised and managed. It is ironical we do not have standardised reference point for measuring the quantum of SR elevation .
This is especially difficult when ST segment blends with forward limb of T waves.
While we have reference point for measuring ST depression (Like during EST ). . . why we do not have one for ST elevation ?
Now we have adopted a rough criteria .Read below .


Posted in cardiology -Therapeutics, Cardiology hypertension, tagged secondary hypertension, tips for hypertension on May 31, 2013| 1 Comment »
95 % of hypertension is designated as primary HT .What does it mean ? It means 95 % of times we do not know what exactly is the cause for raised blood pressure . Simply stated . . . it reflects 95% ignorance .
So what is secondary hypertension ?
Secondary HT is the one, in which we have specific reason for the raised BP. The most important cause is Renal , endocrine etc.
When will you suspect renal HT ?
https://drsvenkatesan.wordpress.com/2010/09/01/when-will-you-suspect-reno-vascular-hypertension/
How is secondary HT different ?
Is stress related HT a form of secondary HT ?
Posted in Cardiology -guidelines, Cardiology -Interventional -PCI, cardiology -Therapeutics, cardiology innovation, tagged banking and cardiac care, cost of ptca, financial issues in cad, funding for cardiac care, insurance ethics in medical care, insurance in cad, ptca by credit, state vs central government spending for cardiology on May 31, 2013| Leave a Comment »
Heart disease was once considered as rich man’s disease . . . It’s no longer true . We in India , are witnessing an epidemic of CAD . The reasons are varied . Apart from conventional factors , social factors like changing demographic pattern , life style , ethnic risk like south Asian metabolic profile are responsible .
While Rheumatic heart disease (RHD ) continues to be a huge burden , CAD is the number one cause for cardiovascular morbidity and mortality .
CAD affect the poor and rich with equal vengeance . The later is better equipped financially to tackle it . Of course , it has resulted in maximum inappropriate interventions. The poor (or borderline poor ) have no other option but to knock the doors of Government hospitals. It is heartening to note, various state Governments are gradually involving insurance schemes.
Still , many struggle to find the required finance for a major cardiac intervention. It roughly costs 100,000 rupees for PTCA .While PCI is required in all symptomatic , critical coronary occlusions , still . . . majority of the CAD in general population do not require it . There are 675 cath labs in India performing 180000 angioplasties every year on an average of 15000 PCI per month ( 500 /day ) This is grossly inadequate . We have huge potential
What is the hurdle ?
No . . . it is all about financial resources
Recently I stumbled upon an advertisement on Times of India

Disclaimer: This article does not in any way defame any hospital that offers the scheme.It just want to debate the concept.
Hospitals want to market the procedure . Convert angiograms to angioplasties . That’s corporate boardroom mantra . And one fine day , bankers and medical doctor sat together and brought a brilliant idea.
Why not do the procedure on credit and push the patient life long into a financial debt !
Wonderful idea . . . many thought .Thus came the financing scheme for cardiac procedures.
Final message
Financing a poor patient with good intention is welcome. But, there is big caveat .In a vast country with high illiteracy , inappropriate procedures may be thrusted upon on the poor souls.
After thought
Now , our patients have one more risk parameter to assess ” Number of remaining EMI( Equal monthly instalment ) and incidence of stent thrombosis” “Accumulated interest and angina” What a wonderful way to provide cardiac care !
I can recall a patient who sold his livestock (his sole income source ) for undergoing a open heart surgery and lost his life as well in the process leaving the family stranded !
Solution
The only solution is to provide a strictly regulated Govt sponsored insurance scheme. High tech procedures should be continuously and meticulously audited for cost effectiveness .
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, Uncategorized, tagged Baseline ECG in the diagnosis of VT, brugada syndrome, epsilon waves in vt on May 31, 2013| Leave a Comment »
Ventricular tachycardia is a common cardiac arrhythmia. The significance of which can be very dangerous to relatively benign depending upon the etiology and underlying heart disease . The ECG during VT is rarely useful to identify the etiology .Often times ECG after reversal will throw more light .
What are the ECG clues one should look for once VT is reverted ?
Posted in Social medicine, tagged accdents as disease, Current events India, ICD code for raod accidents, road accidents as disease, rta as disease, trauma ward on May 30, 2013| Leave a Comment »
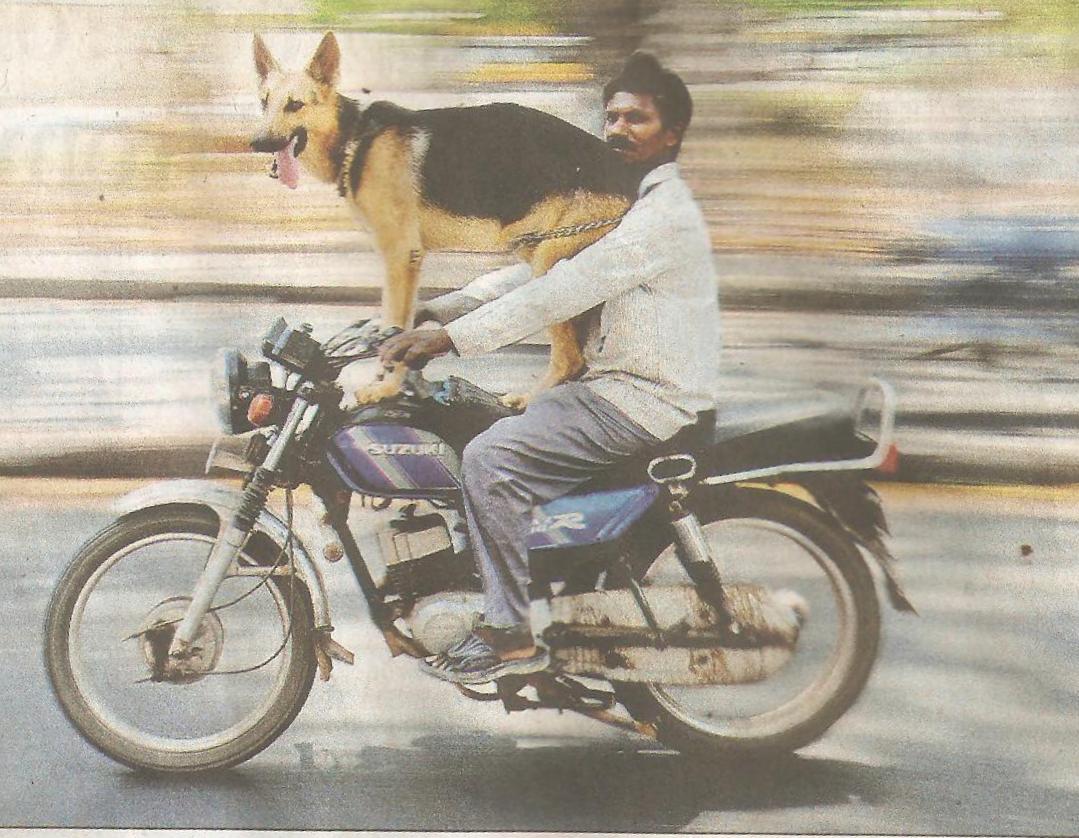
About 150,ooo people die in road accidents in India every year . . . highest in the world ! Myocardial infarction kills only slightly more !
Image courtesy : Times of India , 18th April 2013 . Picture by S.L. Shanth Kumar .
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, Infrequently asked questions in cardiology (iFAQs), tagged endocardial vs epicardial breakthrough, localising VPD, locating the origin og vpd, rv vs lv vpd, septal vpd, septal vpd epicardial breakthrough, ventricular extra systole on May 30, 2013| Leave a Comment »
We are taught in medical schools early in our career , ventricular premature depolarization (VPD ) takes LBBB morphology if it arise from right ventricle , and RBBB morphology if it arise from left ventricle .This is a rough rule of thumb.
Why this rule is unreliable ?
VPDs have a focus of origin—–a short circuit——and an epicardial breakthrough . All these together influence the morphology. Within the left ventricle , a deep endocardial focus can behave vastly different from superficial epicardial focus . The course of VPD is influenced by the myocardial status ( scars etc ) . Further, the electrical properties of interventricular septum is shared by both ventricles .
What happens to a VPD arising from interventricular septum ?
IVS is not only shared by both ventricles , it does not have true epicardial surface (Both side bordered by endocardium ) In most septal VPDs , breakthrough occur on either side of the ventricle . However , It keeps trying to break through epicardial surface ! . Hence , septal VPD is like cat on wall situation .So the morphology varies quiet frequently.Further , the VPD can capture the specialised conduction tissue occurs more commonly with septal VPDs. This can alter both the width and morphology of QRS.




