Archive for March, 2021
Sailing the Osler’s ship of medicine in the third millennium
Posted in bio ethics, Cardiology -Patient page, cardiology -Therapeutics, Clinical cardiology, general medicine, Medical education, Medical ethics, medical quotes, Two line sermons in cardiology, tagged clinical acumen, dr venkat quotes, ethics in medicine, evidence based medicine, guidelines protocols, principles of practice of medicine, rcts in medicine, william osler on March 31, 2021|
Rheumatic fever : Dr Jones would smile if we get rid of the “supportive criteria”
Posted in rheumatic heart disease, tagged acute rheumatic fever, aso titer, chronic rheumatic fever, dr duckket jones, jones criteria, primary vs secondory prevention, rtpcr for rheumatic fever, supportive criteria for acute rheumatic fever essential on March 28, 2021|
Dr. Duckett Jones, the famed American physician, from Good Samaritan hospital, Boston would be a proud man in heaven, to find his criteria still being celebrated all over the globe. He will also be pleased to know his home country USA is painted green on the world RHD map due to his untiring efforts that began in 1944. Of course, what the rest of the world has done in the last century has left us wanting (including the WHO).
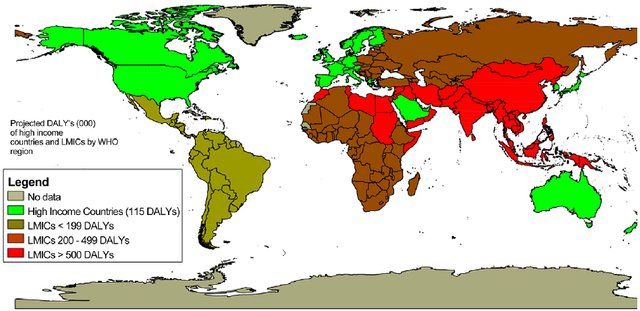
Global RHD map. Note the red and brown shading in south Asia and Africa. It is obvious, RHD is more about economics, equality, and poverty, rather than aggression from an otherwise innocuous microbe called streptococci which is omnipresent all over the world with equal concentration.
How to diagnose Acute rheumatic fever (ARF)?
Simple. Apply jones’ criteria. Funnily, I found it can be a most difficult exercise to do, especially If we realize ARF can defy all the three components it carries. ARF need not be acute, need not have rheumatic symptoms & curiously they need not have fever as well. Did you note this? The entire disease process can be subclinical in 50 % of children. Intelligent patients must realize, how scientifically quixotic conditions we, the doctors are expected to practice medicine.
There is one more ongoing confusion in many of us. Is Jone’s criteria meant for diagnosing the first episode of ARF, or second, or any subsequent episodes? In the strict sense, it can be applied only for the first episode. But it may still help diagnose recurrent episodes. Dr. Jones was so precise in his observation when he suggested the in the later episodes .we may able to diagnose ARF only with minor criteria. But the lacuna here is, recurrent episodes can be so atypical and carditis or chorea may be the only manifestation of that episode making the classical Jones triad redundant.
Someone asked in my class Is there an entity chronic rheumatic fever?
If you describe ARF as a separate entity there must be Chronic RF? logical Isn’t it? . Do you think Jones wouldn’t have thought about this. We don’t know, echocardiography was not even thought of at that time. Better, we stop discussing Chronic RF. (Simply put, all chronic indolent carditis with raised ESR might fit into this imaginary entity)
How important is supportive evidence to Jones’s criteria?
When we have trouble in fixing even the major criteria, where is the question for evidence for preceding streptococcal sore throat come in? By the time we see these children, a throat culture is no longer positive, though ASO titer/Anit DNAse might help. (It must be recalled that culture doesn’t differentiate carrier state from acute infection, a single value of ASO titer ahs little value)
I asked a few of my senior pediatric professors how often they depend (or demand) supportive criteria to diagnose ARF. They agreed in unison, that they never felt the need for it except for academic or epidemiological reasons. When Jones wrote this criterion in 1944, he also never intended to include evidence for previous streptococcal sore throat.
Final message
Is the time nearing to revise Jones’s criteria again and restore with an original suggestion and get rid of supportive criteria? Maybe Dr. Jones wouldn’t object to this as his aim was to tackle a global Pando-endemic rather than worry about few errors of overdiagnosis.
Counterpoint
* For the pure academics, there is exactly the opposite write-up demanding RTpcr to be included as evidence for streptococci sore throat in this site. https://drsvenkatesan.com/2020/10/01/role-rt-pcr-in-the-diagnosis-of-rheumatic-fever-rhd/
Reference

Rheumatic fever: Session 2 Preventive strategies
Rheumatic fever and RHD can be prevented at multiple levels.
Primordial: Preventing all sore throats (that will include Streptococcal ) by promoting social and domestic distancing as we do now for the Novel C pandemic.
Primary prevention: It is about preventing the first episode of RF after getting a sore throat. A course of penicillin after sore throat and trying to interrupt the RF in its incubation period is the aim. I don’t understand why preventing sore throat after exposure to streptococcal droplets doesn’t come under primary prevention too.
Secondary: Preventing recurrent episodes of RF after an established diagnosis of the first episode. ( which of course can be subclinical) This is the classical prevention of monthly injection of benzathine penicillin.
* All levels of prevention activities at the level of the throat. None works in the heart directly.
*Tertiary prevention (Treatment ): It is treating the valve disease and trying to reset the rheumatic clock. Tackling the mitral valve disease with PTMC/MVR is the least economical and most expertise-consuming modality. (Of course more gratifying to both patients and cardiologist) It is all too common even in big tertiary centers do regularly PTMC but shrug off patients from monthly penicillin injections. There should be an in-house responsibility for the cardiologist, that they should ensure at least 100 RHD patients get proper penicllin prophylaxis ( for every PTMC they do)
Which is the best mode of prevention?
Primordial prevention is great. But the best yield will come from primary prevention.If you want to really avoid serious bites on the heart try to protect the heart from the first episode of ARF as the first bite is more intense. To make matters worse, the injury from the first bite is likely to continue irrespective of monthly penicillin.(Karthikeyan G, Mayosi BM. Is primary prevention of rheumatic fever the missing link in the control of rheumatic heart disease in Africa?Circulation. 2009; 120:709–
Can WHO enforce a world microbial order?
One real option that exists, which many feel is artificially stonewalled, is asking vaccine giants like Pfizer, Astra, or BioNtech to fix a deadline and accelerate the process for a global Rhematic vaccine (Wating in the pipeline for 60 years you know) with their newly accrued corona Intelligence. (We have few name suggestions Rhemavax or Rhemshield waiting !)
D-dimer levels in normal pregnancy : Learnt something Important recently !
Posted in Pregnancy and heart, pregnancy and heart disease, tagged fdp vs d dimer, pulmonary embolism dvt in pregnancy, what is the normal d dimer in pregnancy on March 5, 2021|
Have we ever wondered how six liters of blood in our body flows like a live stream, maintaining the fluidity life long, in spite of an active coagulation system in situ, ready to freeze at the slightest provocation (Invisible vascular wear & tear!) This housekeeping job, within the vast network of the human vascular tree, is silently accomplished by a less apparent system called fibrinolytic system. D-dimer is a physiological breakdown product of this system . D-dimer comes from fibrin monomer. The D in D-dimer stands for the domain. (See below) The ability to detect the D-dimer in the bedside has given us a good opportunity to monitor intravascular thrombus formation and subsequent dissolution in health and disease.

Formation of D-dimer from fully formed fibrin clot with the help of factor X111a and plasmin
Learning from a false alarm of pulmonary embolism
Recently I came across a pregnant woman in the third trimester with sudden onset dyspnea. Ongoing panic and a hyper response ER protocol ended up in D-dimer estimation. It was 2600μg/ml, which created a false alarm among obstetricians. She was started on heparin by then. Though her saturation was 95%, ECG was normal.An emergency bedside echo revealed normal right atrium and ventricle, no pulmonary HT. The diagnosis of PE was now rejected confidently. The much-dreaded dyspnea turned out to be some patient anxiety. Unnecessary exposure of a fragile pregnant lady to heparin was reverted with much difficulty as no one was willing to discount jacked-up D-dimer still. (Such is the power of sophisticated biomarkers and numbers! I asked them to report the elevated D-dimer as false-positive in bold letters in the case sheet and applied the break to bring the high voltage obstetrical -cardiac consult to a halt )
What is the normal D-dimer levels in blood?
In the strict sense, D- dimer can’t have normality. It is flushed-out molecular debris from clots, levles of which fluctuates depending upon the fibrinolytic load on a given day. It is further limited by lab standardization issues and methodology. (ELISA vs latex ) Currently, a level of <500μg/ml is considered diagnostically useful to rule out DVT/PVE (Good sensitivity /low specificity)
What happens to D-dimer levels in pregnancy?
D-dimer levels are nornally high in pregnancy, and can reach very high levels as well.
What is this source of D-Dimer In pregnancy?
- Pregnancy is a procoagulant condition. (Estrogen Induced effect on fibrinogen and other clotting factors especially factor 2 & 7 ) We presume it is due to more microthrombus activity in materno placental capillary circulation. When there is a pro-coagulant activity, fibrinolytic activity is also high hence elevating FDP and D dimers.
- Pregnancy-associated with diabetes /PIH/preeclampsia elevate it further due to subclinical endothelial dysfunction
- Placental source for D-dimer is documented. (Might be a marker for partial abruption as well)
- The role of the fetus in generating or triggering maternal procoagulant activity is possible with a reverse breach in the placental maternal barrier. (Many of stillbirth, Intrauterine deaths / DIC in mother could reflect pathological faces of hypercoagulation states)
Normality redefined in pregnancy
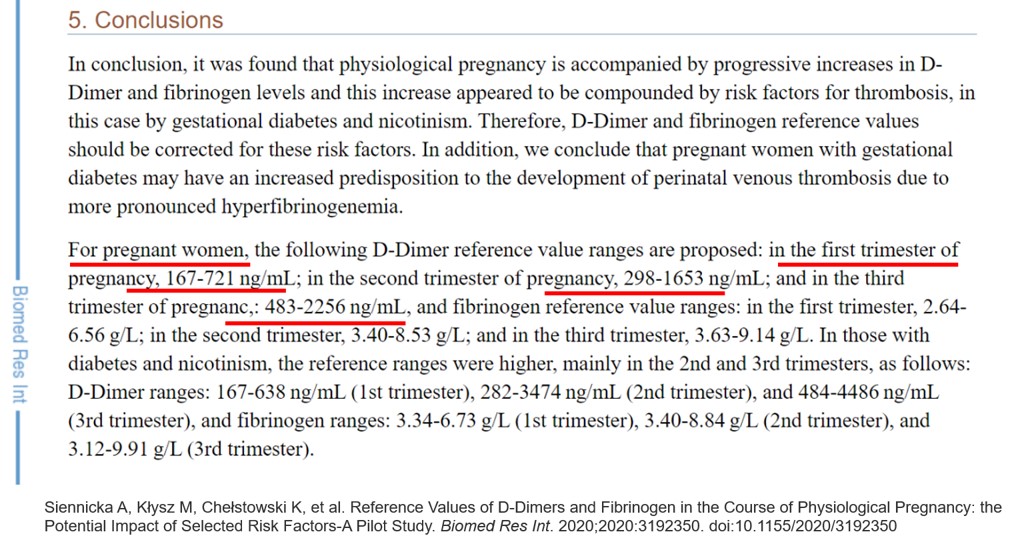
This paper has something important. Didn’t knew this till now. In the third trimester, D-Dimer can reach up to 4400 in diabetic mothers. It is also worthwhile to note the other common causes for high D- dimers sepsis, autoimmune disorders* and occult malignancy,
*In fact, every normal pregnancy can be termed as a relative autoimmune disorder, as it is impossible for the mother to go through the pregnancy without immunological modification of the host (by fetus or host itself)
Final message
Never rely on elevated D-dimer in isolation to diagnose DVT/Pulmonary embolism. This is especially true in pregnancy where even very high levels are physiological. The commonest cause for dyspnea in pregnancy will continue to be anxiety, anemia, PIH & physical deconditioning, and weight gain (not the mitral valve stenosis /PE/or peripartum cardiomyopathy). Yes, It may appear rewarding to think like a specialist, but please realize if we diagnose rare entities, we are “rarely likely” to be correct and the consequences of that are not always pleasant.
Reference
1.Siennicka A, Kłysz M, Chełstowski K, et al. Reference Values of D-Dimers and Fibrinogen in the Course of Physiological Pregnancy: the Potential Impact of Selected Risk Factors-A Pilot Study. Biomed Res Int. 2020;2020:3192350.

Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- August 2026 (2)
- July 2026 (6)
- June 2026 (9)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,716,961 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

