Dr. Duckett Jones, the famed American physician, from Good Samaritan hospital, Boston would be a proud man in heaven, to find his criteria still being celebrated all over the globe. He will also be pleased to know his home country USA is painted green on the world RHD map due to his untiring efforts that began in 1944. Of course, what the rest of the world has done in the last century has left us wanting (including the WHO).
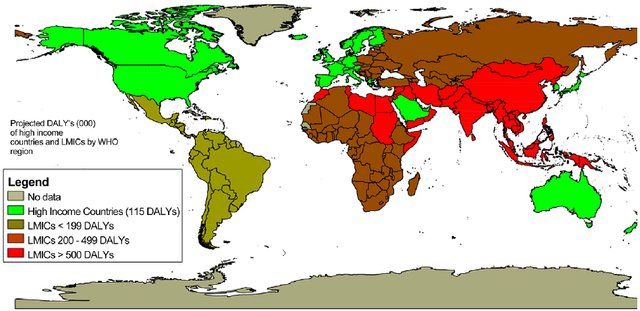
Global RHD map. Note the red and brown shading in south Asia and Africa. It is obvious, RHD is more about economics, equality, and poverty, rather than aggression from an otherwise innocuous microbe called streptococci which is omnipresent all over the world with equal concentration.
How to diagnose Acute rheumatic fever (ARF)?
Simple. Apply jones’ criteria. Funnily, I found it can be a most difficult exercise to do, especially If we realize ARF can defy all the three components it carries. ARF need not be acute, need not have rheumatic symptoms & curiously they need not have fever as well. Did you note this? The entire disease process can be subclinical in 50 % of children. Intelligent patients must realize, how scientifically quixotic conditions we, the doctors are expected to practice medicine.
There is one more ongoing confusion in many of us. Is Jone’s criteria meant for diagnosing the first episode of ARF, or second, or any subsequent episodes? In the strict sense, it can be applied only for the first episode. But it may still help diagnose recurrent episodes. Dr. Jones was so precise in his observation when he suggested the in the later episodes .we may able to diagnose ARF only with minor criteria. But the lacuna here is, recurrent episodes can be so atypical and carditis or chorea may be the only manifestation of that episode making the classical Jones triad redundant.
Someone asked in my class Is there an entity chronic rheumatic fever?
If you describe ARF as a separate entity there must be Chronic RF? logical Isn’t it? . Do you think Jones wouldn’t have thought about this. We don’t know, echocardiography was not even thought of at that time. Better, we stop discussing Chronic RF. (Simply put, all chronic indolent carditis with raised ESR might fit into this imaginary entity)
How important is supportive evidence to Jones’s criteria?
When we have trouble in fixing even the major criteria, where is the question for evidence for preceding streptococcal sore throat come in? By the time we see these children, a throat culture is no longer positive, though ASO titer/Anit DNAse might help. (It must be recalled that culture doesn’t differentiate carrier state from acute infection, a single value of ASO titer ahs little value)
I asked a few of my senior pediatric professors how often they depend (or demand) supportive criteria to diagnose ARF. They agreed in unison, that they never felt the need for it except for academic or epidemiological reasons. When Jones wrote this criterion in 1944, he also never intended to include evidence for previous streptococcal sore throat.
Final message
Is the time nearing to revise Jones’s criteria again and restore with an original suggestion and get rid of supportive criteria? Maybe Dr. Jones wouldn’t object to this as his aim was to tackle a global Pando-endemic rather than worry about few errors of overdiagnosis.
Counterpoint
* For the pure academics, there is exactly the opposite write-up demanding RTpcr to be included as evidence for streptococci sore throat in this site. https://drsvenkatesan.com/2020/10/01/role-rt-pcr-in-the-diagnosis-of-rheumatic-fever-rhd/
Reference

Rheumatic fever: Session 2 Preventive strategies
Rheumatic fever and RHD can be prevented at multiple levels.
Primordial: Preventing all sore throats (that will include Streptococcal ) by promoting social and domestic distancing as we do now for the Novel C pandemic.
Primary prevention: It is about preventing the first episode of RF after getting a sore throat. A course of penicillin after sore throat and trying to interrupt the RF in its incubation period is the aim. I don’t understand why preventing sore throat after exposure to streptococcal droplets doesn’t come under primary prevention too.
Secondary: Preventing recurrent episodes of RF after an established diagnosis of the first episode. ( which of course can be subclinical) This is the classical prevention of monthly injection of benzathine penicillin.
* All levels of prevention activities at the level of the throat. None works in the heart directly.
*Tertiary prevention (Treatment ): It is treating the valve disease and trying to reset the rheumatic clock. Tackling the mitral valve disease with PTMC/MVR is the least economical and most expertise-consuming modality. (Of course more gratifying to both patients and cardiologist) It is all too common even in big tertiary centers do regularly PTMC but shrug off patients from monthly penicillin injections. There should be an in-house responsibility for the cardiologist, that they should ensure at least 100 RHD patients get proper penicllin prophylaxis ( for every PTMC they do)
Which is the best mode of prevention?
Primordial prevention is great. But the best yield will come from primary prevention.If you want to really avoid serious bites on the heart try to protect the heart from the first episode of ARF as the first bite is more intense. To make matters worse, the injury from the first bite is likely to continue irrespective of monthly penicillin.(Karthikeyan G, Mayosi BM. Is primary prevention of rheumatic fever the missing link in the control of rheumatic heart disease in Africa?Circulation. 2009; 120:709–
Can WHO enforce a world microbial order?
One real option that exists, which many feel is artificially stonewalled, is asking vaccine giants like Pfizer, Astra, or BioNtech to fix a deadline and accelerate the process for a global Rhematic vaccine (Wating in the pipeline for 60 years you know) with their newly accrued corona Intelligence. (We have few name suggestions Rhemavax or Rhemshield waiting !)



