This is a re-blog from 2010 pages of this site.
Hope we have more updates.Spouse behaviour as significant CAD risk factor, is still a valid research concept that shall lead to more productive social “cardiac Interventions” and prevent CAD burden outside the much glamorised cathlab
American journal of epidemiology in a land mark analysis has found , spouses share the same profile of coronary risk factors .This is a huge finding , considering the fact that , genetic factors are not involved here . So , it is something to do with family diet ? domestic issues, sibling effect ?
It is well-known lipid profile of family members are comparable . There are many Indian families who have high basal triglycerides .Mind you, husband and wife is the least (Zero link) linked genetically for familial dyslipidemia ,still they often share a similar lipid profile
Related issues without answers !
When a spouse gets a coronary event what are the chances of other to develop an event ?
Any body’s guess
In this era of bi- polar family life, can spouse behavior /unrest be a coronary risk factor ?
Exclusive plant based diet protects heart and vasculature. Is it true ?
“Yes it is.“
“No, It doesn’t.“
“Yes, a little bit”
So, the answer is not stright-forward. Then as a scientist what should we do ? Do some good studies.
Do we have it ? Ofcourse, we have far too many to confuse us.
Which study showed vegetarians has less risk of CAD than non vegetarians?
There have been several studies that have explored the association between vegetarian diets and the risk of coronary artery disease (CAD) compared to non-vegetarian diets. While not all studies show consistent results, some research suggests that vegetarians do have a lower risk of CAD. Here are two examples from heap of research on this topic.
The Adventist Health Study-2 (AHS-2): This is a large prospective cohort study that included more than 73,000 participants, including both vegetarians and non-vegetarians. The study found that vegetarians had a lower risk of hypertension, diabetes, and metabolic syndrome, all of which are risk factors for CAD. The results also indicated that vegetarians had a lower risk of heart disease compared to non-vegetarians.
EPIC-Oxford Study: This is another large prospective study that included over 45,000 participants in the United Kingdom. The study compared the risk of CAD between vegetarians and non-vegetarians and found that vegetarians had a lower risk of heart disease.(EPIC -OXFORD long term follow up 2022 available Ref 2)
Post -research sequale
Does every one agree with these studies ?
The answer is “No” again
Why ?
There are three issues come to my mind
1.First of all, we have a problem in defining not only the CAD* but also who is a pure vegetarian and who is an impure non-vegetarian. (*Clinical vs. nonclinical, ECG or CAG-based, etc.)
2.There are too many parameters, both endogenous and exogenous, that determine the incidence of CAD. This can pose a real challenge to any sophisticated logistic regression model. This includes epigenetic, food, and atmospheric interactions with the endothelium. Technically, if you were to include polluted air as a bad diet equivalent, it would make things really difficult for the poor research fellows.
3. Finally, our understanding of the difference between cardio-vascular risk factor vs acute trigger (both emotional or physical which actually precipitate the event.) , is not perfect, These can profoundly influence the true Impact of diet over CAD and throw the results of all these studies topsy turvy.
Final message
Pardon me, for some confusing content in the post .I go with with EPIC-OXFORD conclusion. Plant based diets are indeed CAD protective. As someone said, everyone would like the right answer to be linked to their belief system, whether humans are really herbivores or not.
“Observe your thoughts,don’t believe them” Eckhart Tolle
High value
1.Pacemaker & Defibrillator
2.Heparin in Acute coronary syndrome
3.Diuretic therapy for cardiac failure & pulmonary edema
Low value
1.PCI> 24 hrs after STEMI
2.Most CTO Interventions
3.AF ablation
Strong contenders for high value Interventions
1.PTMC
2.Thrombolysis & DAPT
3.Diet and excercise modulation
Strong contenders for low Value Intervention
1.TAVI in young & SAVR eligible population
2.Mitra clip
3.LAA appendage closure
Final message
Unfortunately, most of us are blinded (artificially though!) to quality check , outcome assessment, & comparative effectiveness with already available treatment modalities.Every cardiologist shall create their own value based list of intervention according to their conscience, and stick it on the consultation table as a ready recokner.
Counterpoint
Value is a subjective concept that can be challenging to define precisely. It may not always apply equally to every individual.Ideally, population based value assessment should give us the true value. Reality is different. In some cases, what may seem like nonsense to others can hold significant value for a particular person. This highlights the importance of recognizing diverse perspectives.
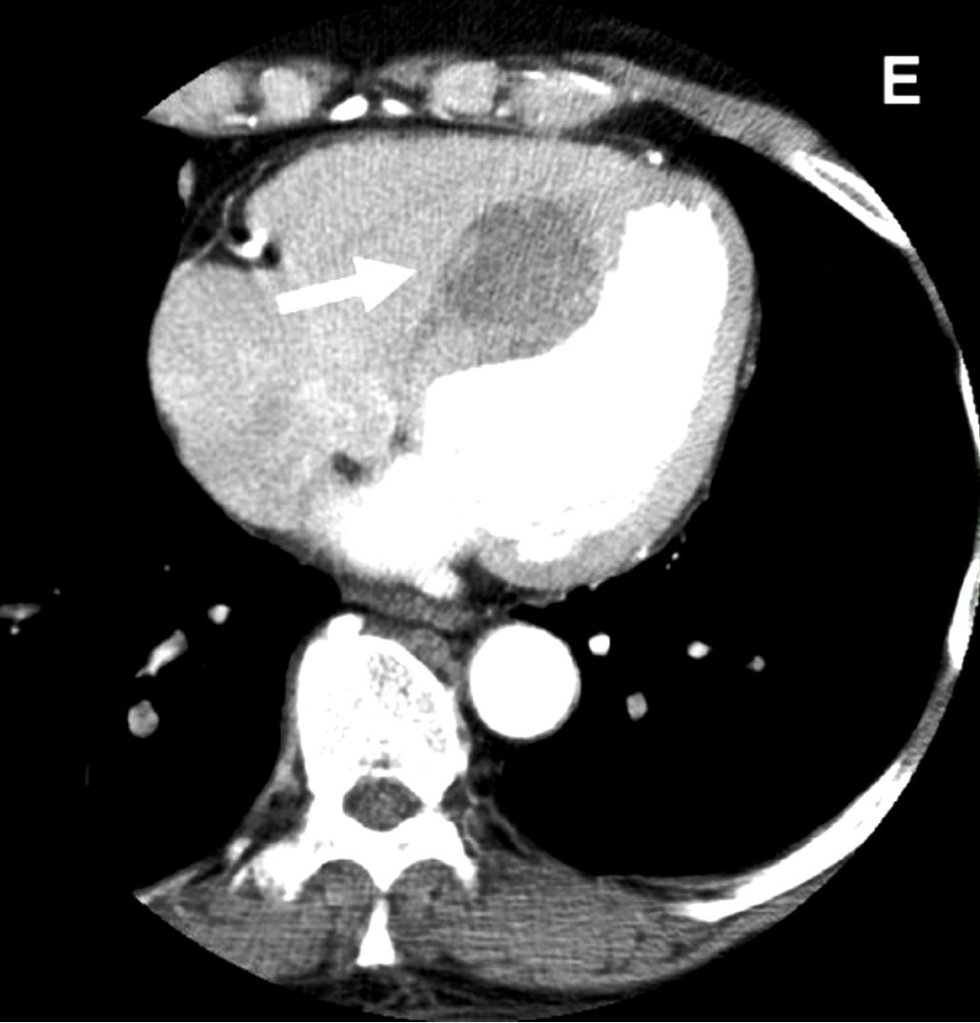
It looks like an Intracardiac tumor, a myxoma ? a variant of HCM ? Is it a hydatid cyst, ?
No it’s not. I can give one clue. This is a man-made condition.
Oh ok, did this happen inside the cath lab ?
Yes, you got it, right. But need a diagnosis.
Can you give me one more clue?
This patient was undergoing PCI for chronic total occlusion.
So, it must be a complication. Then I need to know the list of complications during CTO PCI.
Yes, but you may not find this one in the conventional list. Let me come out with the answer.
Answer
It is a huge septal hematomadue rupture of vulnerable septal collateral during retrograde wiring for opening LAD CTO.It usually occurs due to o prolonged procedures and hardware-related injury. Thanks to the authors from Taiwan to post this case report. (Image Courtesy Lin & Wu 2005 Ref 1)
Lessons from this case report (Not meant to offend anyone )
This case gives us some important lessons to be learned. One of my senior colleagues used to say, opening a CTO is ok, but using a retrograde approach with aggressive deploying of hardware within the last remaining lifeline provided by the donor coronary artery is a culpable coronary crime unless it is a life-saving procedure.
The often used term “septal surfing” adds an “adventure sport feel” to our youngsters posing as an interventional challenge and amplifying the potential injury. The fact that epicardial collaterals have a larger caliber, but the temptation to cross it, is significantly suppressed (or even forbidden) due to the risk of tamponade. However, this doesn’t in any way give us the freedom to toy with septal collaterals. Proliferating hardware (Innovative though ) is also an issue. It is true, technological input is a pillar for the growth of science. However, it is a sad fact, many of us are compelled to learn risky, unscrutinized tricks exclusively from academically unbaked industry guys, rather than from mainstream literature.
Final message
“No procedure … no complication”
I could recall, one of my colleagues displayed this caption as the last slide in a cath lab workshop, after a talk on How to avoid complications in the cath lab.
Very true. But, CTO by itself never belongs to a malignant subset of CAD, as some sections of the cardiology community would want us to believe. CTOs do need an intervention, only as a life-saving /0r severe symptom-relieving procedure. Most of them aren’t. They present with stable angina because of extensive collaterals. Unfortunately, instead of respecting this, many of us are asked to close these channels and try to maintain antegrade flow. The irony is, to open the CTO we may end up sacrificing these life-saving channels.
If you think this quote is too brutal, please visit the Nobel laureate Initiative “Lown Institute” website and spend some time, to find solutions to rescue the medical profession, which is rapidly drowning in a sea of ethical dysfunction.
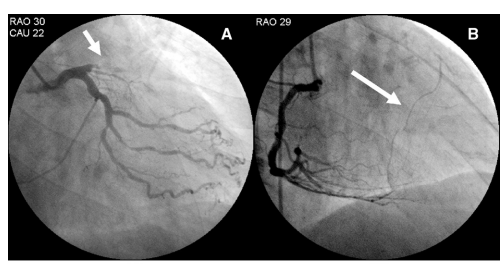
A simple question with mammoth repercussions in the revascularization world.
How was the question ? Was it difficult ?
Don’t worry, it wouldn’t be the same even for elite cardiology experts worldwide. It is not a Himalayan task, though, to find an answer. All it requires is a simple FFR run through pre and post PCI (Now RFR, iFR, QFR). Surprisingly, very few inquisitive minds wanted to do this. I can find 5 related papers. The fifth one is very specific: REPEAT-FFR study. Go through at least that one paper and find the answer yourself.
Cardiology fellows it is worth reading about this important study , might be asked in exams.
Final message
The conclusions from these studies are not really baffling, but demand a lot of academic cleansing of our understanding about the relationship between epicardial patency and microvascular flow.”It is obvious from these studies that epicardial PCI never guarantees good revascularization with a FFR backing “
Every cardiologist should ask this question before they scrub, whether the PCI, they are going to do today, would improve the net-myocardial flow, LV function or symptoms . Are we doing justice to our patient (or blindly practicing science) who is quietly lying on the table, with a mix of anxiety and trust, with a complete belief that what they are undergoing is a life-changing or life-saving procedure.
Further, it is our duty to restore the lost glory to the defamed , stigmatised medical management of CAD & Impress our patients that “All that, doesn’t glitter could be pure gold as well”
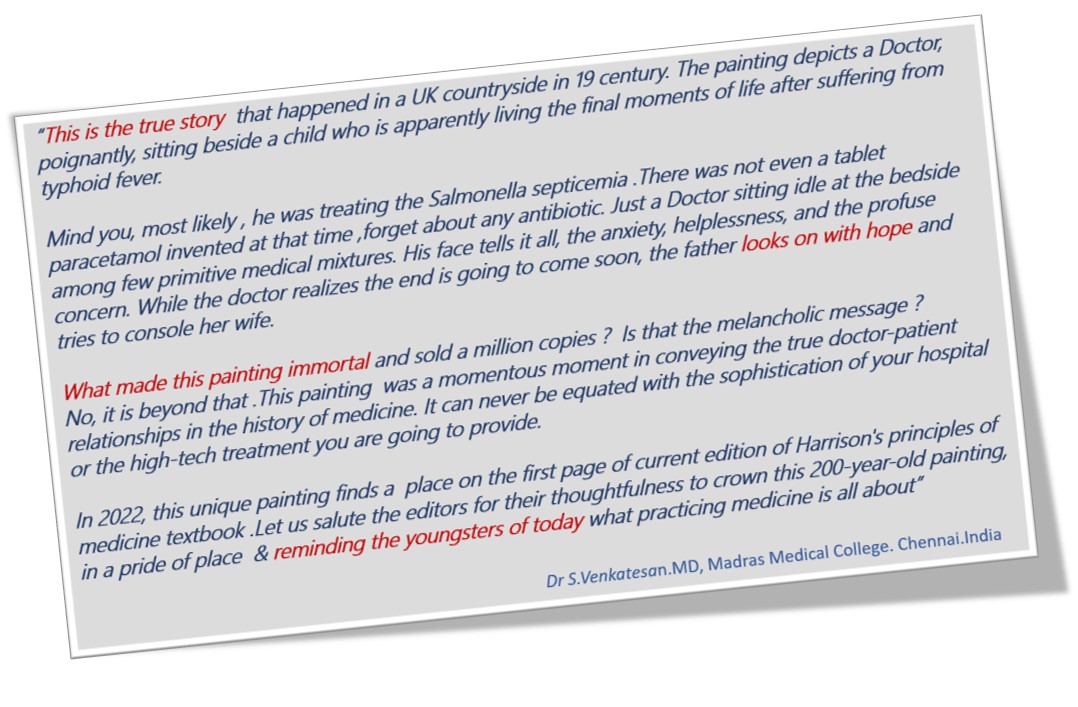
No medical painting Impacted us this much. “The Doctor““was exhibited in 1891 by Sir Luke Fildes and Presented by Sir Henry Tate in 1894 in London. I am sure most of us are aware of this painting. Sharing it for future generations. Wish, this painting is embedded permanently in every young medico’s nimble brain.
This painting soulfully pours the silent and sacred bond between a helpless doctor and his dying patient, , which happens to be a lovely child.
Anyone who is flushed with millions can become a member of “The Hurlinghamin” London or the “Yacht” in Monaco, or any other glamorous clubs in the world. But, EBC* is different. Only cardiologists are privileged to enter. EBC is obviously unique. It is the only club addressing exclusively a subset CAD, ie bifurcation coronary lesions. Apart from immense pride and academic entertainment, it teaches us some deep technical points. (By the way, BFL* is a minuscule spoke in the gigantic wheels of global atherosclerosis)
Approach to BFL
90% of BFL still require only drugs or humble single stent or a provisional second stent strategy. However, as per basic rules of human intellect, lesser problems continue to bother us and consume our precise time. This continues, even after realisng , there are 6 complex two stent strategies that doubles up complications.
(*EBC -European Bifurcation club .BFL-Bifurcation lesion)
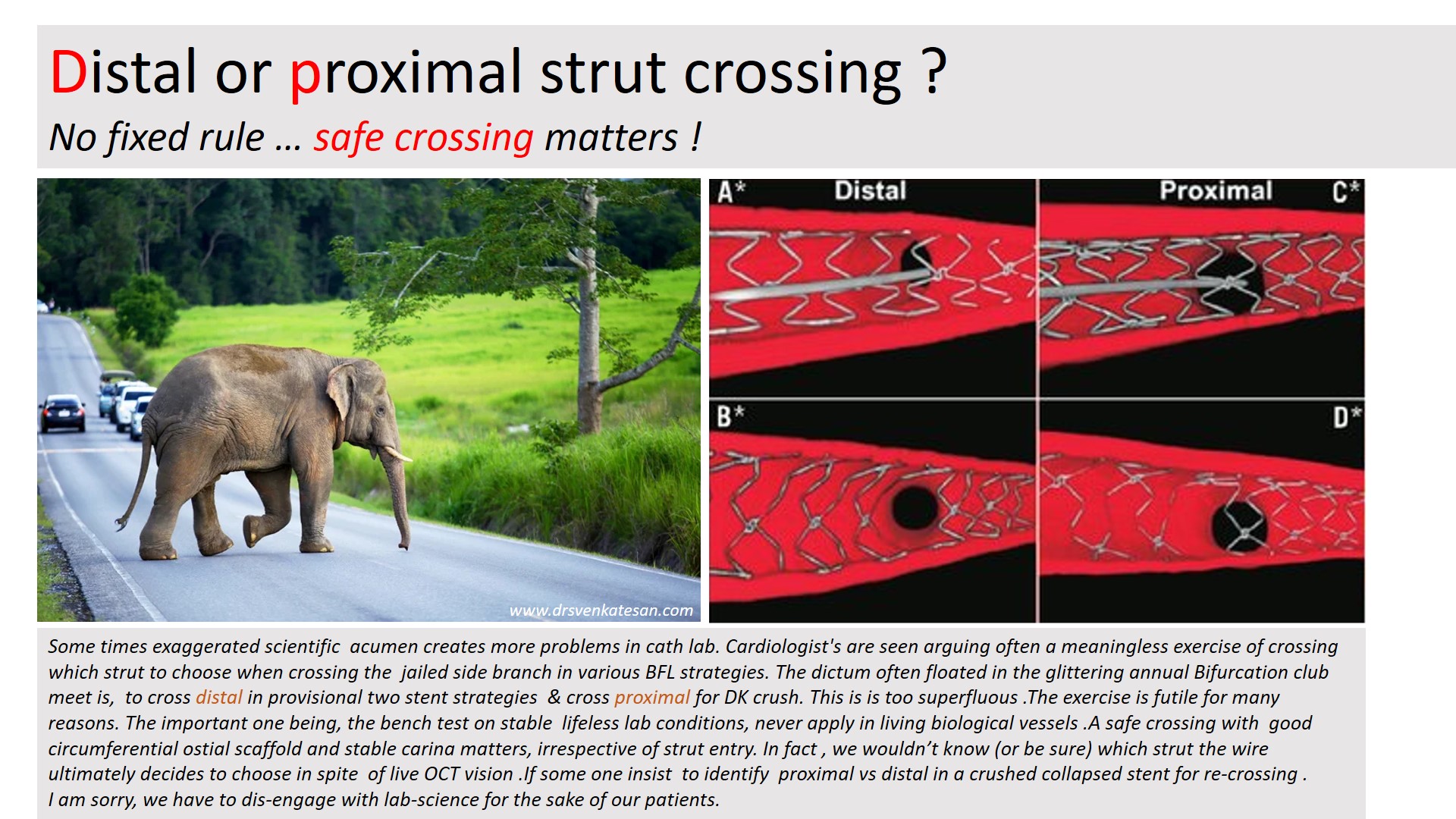
We will address one unique issue in BFL. May not be a major clinical issue .Still, it’s worth it. It is about the side branch crossing after the intentional jailing of the side branch.
Let us answer this query first
Pure science: Observations from Bench test (Text from Ref 1)
In contrast to provisional stenting in which re-crossing through a distal strut is desirable, initial re-crossing the crushed SB stent in the DK crush technique should be done through a proximal stent strut to minimise the risk of SB stent deformation. A theoretical exception could include bifurcations with a particularly narrow angle for which proximal re-crossing may shift more struts towards the MV, leading to a less desirable, longer neocarina. The 2nd recrossing should be done through a distal strut.
Bench testing is clear. Still , Why this confusion ?
We are all talking about theory in bench testing in stable non-hemodynamic conditions that lacks a biological carina and the dynamics of plaques. We are aware that there are at least 5 virtual ostia in every bifurcation arena (or trifurcation) . The qunatum and direction of plaque sharing occurs with a random effect. We also know the final kissing either cements these plaques perfectly or unsettles in a most bizarre way. So, these strut crossing stuff, are more of an imaginary bio-engineering principles. Whichever strut you cross, do it slowly, gently dilate it to the maximum within the polygonal confluence and good approximation. Don’t get too much carried away , even live online OCT guidance do not guarantee a perfect crossing.
Final message
The answer to the title question seems to be (me), one need not hair-split much on the site of crossing at the side branch. Fortunately, in whatever way, we weave the metallic mesh*, at the epicenter of the coronary highway, it is the natural secretagogues like TPa, Nitric oxide, PGI-2, along with DAPT decides the patient’s genomic fate.
*An appeal to all EBC club members.Before embarking upon a compex PCI on a stable patient , please think for one last time , whether your patient might do well, only with medicines.
Referecne
1.Hall AB, Chavez I, Garcia S, Gössl M, Poulose A, Sorajja P, Wang Y, Louvard Y, Chatzizisis YS, Banerjee S, Xenogiannis I, Burke MN, Brilakis ES; Collaborators. Double kissing crush bifurcation stenting: step-by-step troubleshooting. EuroIntervention. 2021 Jul 20;17(4):e317-e325. doi: 10.4244/EIJ-D-19-00721. PMID: 32310131; PMCID: PMC8919516.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.