Coronary Imaging : OCT works only in OCTOBER ! What to do in other months !
— Dr.S.Venkatesan (@VenkatThoughts) August 29, 2023
ESC 2023, throws silently two spanners( ILUMIEN 4, & OCTOBER) into the confused cath lab corridor ! https://t.co/GLwdz6tOV5 via @VenkatThoughts
Archive for August, 2023
ESC 2023 : Coronary Imaging update
Posted in Uncategorized on August 29, 2023|
New ESC 2023 Cardiomyopathy guidelines: Truths trail by 17 years!
Posted in cardiomyopathy, Dilated cardiomyopathy, hypertrophic cardiomyopathy, ischemic cardiomyopathy, Uncategorized, tagged drsvenkatesan, ESC 2023 new cardiomyopathy guideline, ndlvc, non dilated cardiomyopathy on August 27, 2023|
It was 2006
Allow me to recount an unassuming piece of a PowerPoint presentation from my institute, Madras Medical College, at the annual Cardiological Society meeting in New Delhi. The paper was categorized under miscellaneous sessions. I vividly remember the day. I have to admit, It was a nearly empty hall E, located in the basement of Hotel Ashoka. After the talk, I looked up to find that neither the chairman nor the handful of kind academic souls had any questions or comments to make. Pausing for a few moments, I quietly walked down the podium with an inexplicable silent pain.
The title of the presentation was “Non-dilated cardiomyopathy”
Welcome to ESC Congress Amsterdam August 2023
ESC, has come out with this new update on cardiomyopathy. It is a pleasant surprise to find the term “Non dilated cardiomyopathy” entered the cardiology academia, authenticated by the ESC.
I must confess, it is difficult to conceal the joy and a little bit of self-pride.
Some observations from this document
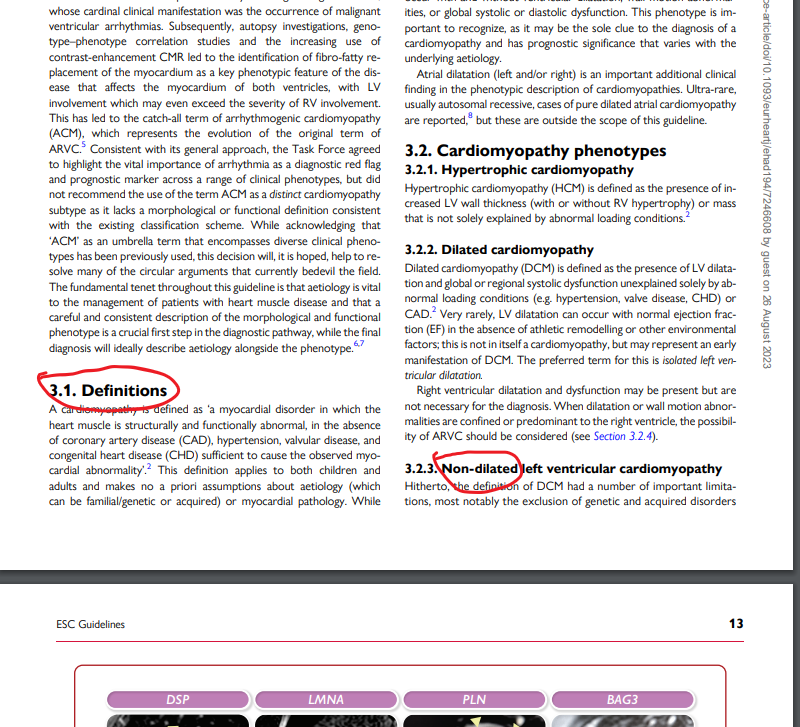
1. Despite our tremendous knowledge base, we are yet to hang up our boots, in pursuit of an Ideal cardiomyopathy definition. Genotypic or phenotypic ? Phenotype is closer to reality, while genotype is largely imaginary. It looks like, The newer guidelines are moving towards a phenotype-based approach in all aspects except in risk prediction. Fair enough.
2. All cardiomyopathies, whatever way we segregate, ultimately end up in the common clinical syndrome of heart failure. So. it is better to spend some quality time here and concentrate on HF therapeutics.
3. Cardiologists are expected to critically fine-tune their general medical knowledge, which will help recognize and treat systemic disorders like Amyloidosis, and other metabolic infiltrates.
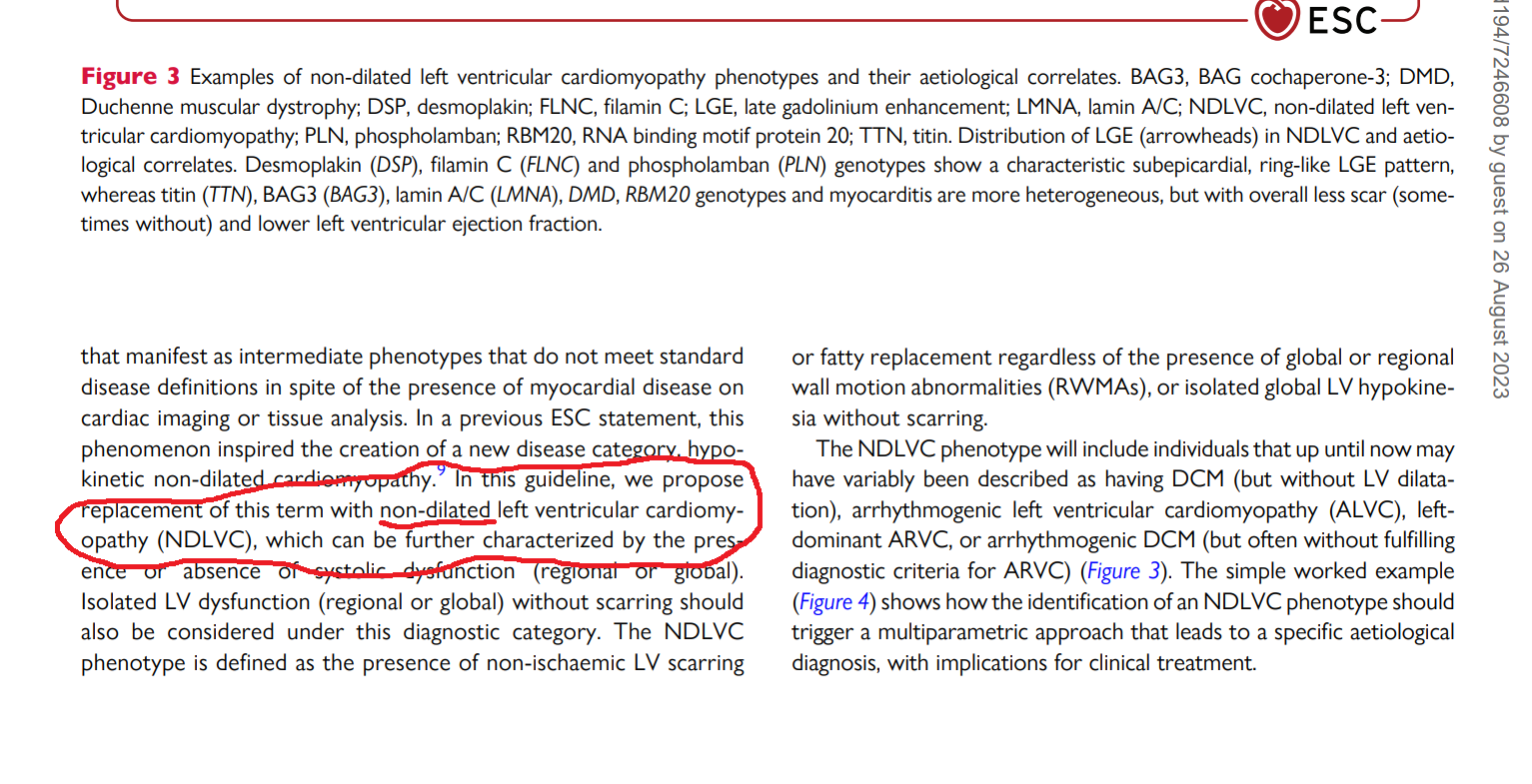
4..Almost all RCMs have non-dilated ventricles, so why a new term NDLVC? Anyone wants to ask this question ?. Further, there can be significant overlap between RCM & NDLVC as well. Definitely, there is a lot to understand beyond this 2023 document.
5. Why do some ventricles refuse to dilate even in the face of adverse hemodynamic and pathological conditions. Is it an advantage or disadvantage? If ventricles are adamantly stiff and decide not to dilate, there is no other option, the atria will proxy dilate, creating more problems in the lung circuits. This also raises a fundamental question Is NDCM a better stress buster (think Laplace law ) than DCM? or vive versa , the accomodative nature of LV passify & blunt the slope of LVEDP at times of exertion.
6. One more reality is, NDLVC is also an Important subset in the now fashionable HF entity HFpEF
Final message
The message to youngsters is this. Discuss, debate, and document your thoughts in whatever forum, that is available. Don’t wait for all those big brother journals and their recognition. If there is truth in your writing, someday it will be revealed to the world.
Reference
Best excercise for optimal BP control : A meta-analysis & a surprise conclusion !
Posted in Uncategorized on August 26, 2023|
Lifestyle modifications and non-pharmacological modalities should be started in every hypertensive individual before starting them on long-term drugs. This is one of the foundational lessons in the therapy of hypertension. (Please mind, in no way, it conveys a meaning that we can give less importance to them after starting drugs.)
Exercise prescription has become a big-ticket event in hypertension clinics in recent times. Though any physical activity in adequate quantity is good, we have classified exercise into complex subtypes and found fancy ways of its administration.
Traditional belief gets a kick-back
We (At least me!) have been taught, isometric exercise is not BP-friendly. In fact, it can cause intermittent spikes that may persist for a variable duration depending upon the basal as well as dynamic adrenergic vascular tone. This is what I had taught to my students. This presumption is nearly shattered by this meta-analysis. It concludes that among all, Isometric exercise reduced the BP more than others. (especially wall squats and planks). More surprising is, that the usefulness of aerobics is lesser than dynamic resistance training as well.
Final message
Contrary to popular belief, Isometric exercise is not really hard on blood vessels and is likely to have a more favorable effect on blood pressure than aerobics.
Still, hesitating to fully accept the conclusion of this study. Exercise prescription is highly individualized & includes multiple cross-over strategies and self-learning. Caution is required when doing strong isometric exercises, especially after a vascular event.
Reference
A simple tip for peace of mind … for the modern patient
Posted in patient education, tagged ai in medicine, faith trust in doctors, patient behaviour, patient empowerment, technology in mediine on August 20, 2023|
Preamble
A patient who had a PCI some time back , asked me in one of his recent visit.
Doctor what is microvascular endothelial dysfunction and erosison ? Am I at risk of developing it ?
What am I supposed to answer ? Yes, I some how managed .” Don’t worry , it is a complex biological phenomenon. you need not go deeper into that. Take medicines regularly” He wasn’t happy with my answer is a different story.
A simple tip for peace of mind … for the modern patient
If the current generations of patients , equipped with hyper-knowledge engines, insist to understand 100% about their illness, imagine the consequences to the global healing system ,that has so many ground level issues to bother about.
One unofficial estimate from an elite , professional academic chatterbox of medicine suggests that the knowledge base with which doctors diagnose, treat, and understand the diseases they tackle, is at best 15%. Pateints need not be thankful , but atleast understand we are for working around with 85% ignorance, and still tries to bring out the best. I am sure this is a fact, no one can disagree ,regardless of the presence or absence of evidence to support it.
Final message
It might appear fair if someone argues blind faith in a trusted physician or hospital could end up as unscientific or unethical. But,what they fail to realize is, sciences’ blindness can be much darker, especially when it comes to the outcome of treatment and prognosis.
What does statin do to Cholesterol absorbtion from Intestine ?
Posted in Uncategorized on August 19, 2023|
Does this sound a difficult question ? Many felt so. Hence, I decided to chat with the popular AI machine.It is a brief little chat that surprised me .Please click the link , you can learn somee academic manners from the machine.
https://chat.openai.com/share/6b96c54e-ad52-472a-9ebd-b7b1e1c762be
Statin: Some untold story.
Last century’s rockstar drug, statin do stimulate cholesterol/sterol abosorbtion as well as possible neo-hepatic synthesis.This is basic bio-feed back mechansim , when one molecule is blocked in a living organsim. We must be aware, It is a less popularised truth (Intentionally ? ) among the cardiology community,
Ofcourse LDL comes down, at the cost of residual pre -choleterol particles that spill over to circulation resulting in hepatic and skeltal muslce injury.
There is an important corollary and a pharmacological cross invention and a new big market for a otherwise orphan drug called Ezetimibe.
It is not an optional accessory in statin therapy as many would like to think. There is good scientiifc logic, with and and without evidence though , that Ezetimibe, is an essential add on adjuct for optimal statin action.This is understandable, since statin consumption systematically depletes intracellular cholesterol, make the entire small intestine hungry for cholesterol by a bio – feed back mechansim once its synthesis is blocked.
There is also some concern liver might also synthesise some abnormal new unnamed lipids ,? as its normal cholesterol pathway is blocked. These info were never released to clinical domain.
Final message.
Statin tiggers increased lipid absorbtion at the intestines. Stand-alone statin therapy, still turns out to be a suspect value in atleaset one third of users as the bio -feed back surge could not be countered effectively. However, for statin to be optimally effective,add on Ezetimibe helps.
Also, It is clear one of the important duties, of medical professional is to teach the AI engine and help correct potential and real mistakes in its data base.
Reference
This is evidene less cardiology , ie class C evidence.Experts may add, dispute and contibute to this thread.In the process Chat GPT might learn as well.
Found one evidence
I am 49 … not out, how about you TAVI ?
Posted in Uncategorized, tagged prosthetic aortic valve, starr edwards valve, tavi valve on August 1, 2023|
This post was written after coming across a case report Oxford medical case report.


What is the life of a prosthetic Aortic valve?
The standard answer needs to be, mechanical valves can last up to 25 years or more. But, we are in a techno-conflict era. Instead of working on the longevity of the valve, ( with concerns for long-term OAC ) we fell for the biological valves. Curiously, this has made the durability of the valve, a less relevant discussion in many centers. We get excited when some company brings out a long-lasting bio-prosthetic valve that can live up to a maximum of 15 years.
Now, the biological valve comes in a new avatar ie TAVI, in a big way. Soon, we may celebrate an event free 10 years after TAVI. Going percutaneous is transformative. But at what cost? Fusion of metallurgy, chemistry, and pharmacology should make it possible for in-vivo metal valves to be safe for 75 years of human life span. The irony is we almost had one, One valve’s longevity was consistently exceeding the patient’s life span,(at least as far as we observed in the Rheumatic heart disease) This has been the star of all valves. We know what happened to that valve.
This SE valve in the mitral position
Final message
Most SE valves are implanted in the mitral position. Starr-Edward in an Aortic position working for 50 years is a big proof of reality. Of course, we can’t extrapolate with a single case report. We have stopped the production of these valves. So, there is no way to test it either. Anyway, cardiologists, cardiac surgeons, and finally the generation X, TAVI Innovators have something to learn from this case report. Forget Starr-Edwards, It looks like, there are some invisible forces that work against mechanical valves in recent times, which may not be good for our patients as of now. (There is something interesting related to this in Ref 2)
Future directions: Past need not be past
Nothing is impossible for our hyper-talented scientists, except probably in the “faculty of looking back” the past-Innovations (falsely labeled as obsolete) and bringing them again to optimal usage. If cardiologists feel surgical AVR injures their interventional pride, how about a percutaneous cage delivered at the root of the aorta, after ablating native leaflets, followed by an inflatable silicone ball?
Reference
A current 2023, opinion from the renowned Dr. Catherine Otto on this Mechanical vs biological valve , Indications, current usage pattern, the cut-off age, etc
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- August 2026 (2)
- July 2026 (6)
- June 2026 (9)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,716,053 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

