This question might squeeze the collective coronary knowledge of any cardiologist. (At least, it does for me !)
What is an intermediate coronary lesion? (ICL)
Traditionally it is an “angio-ocular reflex” measurement of coronary arterial diameter stenosis that lies between 40 to 70% (Mind you, 70 diameter stenosis is 90% area. So, we must be clear what we really mean in any revascularisation debate).
Above one is the simplest expression of ICL. (* While 70% cutoff is fairly constant, the lower limit 40% is still not a settled issue. It can be 30 or even 50 %. I think we haven’t yet named the lesions 1 to 49 %. It is the spectrum that contains Coronary erosions, ulcers, luminal irregularity, or the evasive term minimal CAD )
Many sub-classes exist in ICL.
- Should ICL definition be different in proximal LAD? (A 40% PDA or OM2 lesion is not the same as 50% LAD right.Maybe we need to artery specific redefinition, left main we did it already)
- It can be de nova chronic (most common ) Acute /subacute, acute recanalization (Each has a different management strategy)
- What about ICL with good TIMI 3 flow. Mostly safe and can be ignored?
- Should we bother to know the content of ICL? It could be a minor plaque or just thickened and narrowed arterial wall or even layered thrombus.
- Is it isolated ICL? When ICL occurs in isolation it gets more attention is natural to ignore if ICLs are noted along with other critical lesions nearby. The risk of ignoring or risk of including ICL in the final angiogram reports is unquantified.
- When two ICLs lie by next to each other (Tandem ICL) will you add the stenosis resistance in series? Does the length matter.(Can we measure net FFR ?)
- Is it symptomatic vs asymptomatic? (very difficult query )In stable non-Infarct CAD Internedaite lesions do not obstruct flow, but Post ACS it is the distal microvasculature that determines the epicardial flow. so even intermediate lesion resist flow.
- ICLs in ecstatic segments pose a special issue. Adding to this Galovian positive remodeling mask the true plaque burden(Currently liberal use of OAC like warfarin are used in ectatic vessels with ICLs)
- By the way, is it true, ICLs are more prone for ACS? We believe it based on small studies and sort of biased teaching. Of course, there is some truth in it, but in a larger sense, it is not correct thinking. ICLs by sheer number overtake the critical lesions in terms of Incidence. So more ICLs present as ACS. But in, pure pathological terms flow-limiting lesions do carry more risk for ACS. (Of course, calcification might stabilize a few of them, and convert them to CCS) . For argument’s sake, if we agree ICLs are more prone for ACS, we should first fix these lesions than the more tighter ones.(Any guidelines forthcoming ?)
- Finally, the most important query Is the ICL vulnerable, or is it flow-limiting? (read below)
Imaging and physiology
CAG is just a shadow of contrast luminogram. Further, the contrast flowing across a lesion cannot be equated with the true velocity of blood flow. So, what shall we do? How do we overcome the limitations of CAG shadow? We need to go after more glamorous shadows like IVUS and OCT. They do suffer from myopia and hypermetropia respectively. Still, they are good enough to reveal important info like the content of lesions like calcium thrombus with acceptable precision, etc. The thickness of the fibrous cap (TCFA) is a current marker of vulnerability. This thickness is dynamic as do plaque liquefaction. We are looking ahead to the days of virtual histology and plaque metabolism by NIR spectroscopy. Decisions based on a single one-time snapshot from intermediate lesions would largely be meaningless.
What about physiology? FFR, iFR,(Adenosine free) QFR (Based on TIMI frame count) offer a more scientific assessment of flow across the lesion. Still, it is not clear. An elegantly made study is available that depicts the relation between stenosis and FFR.
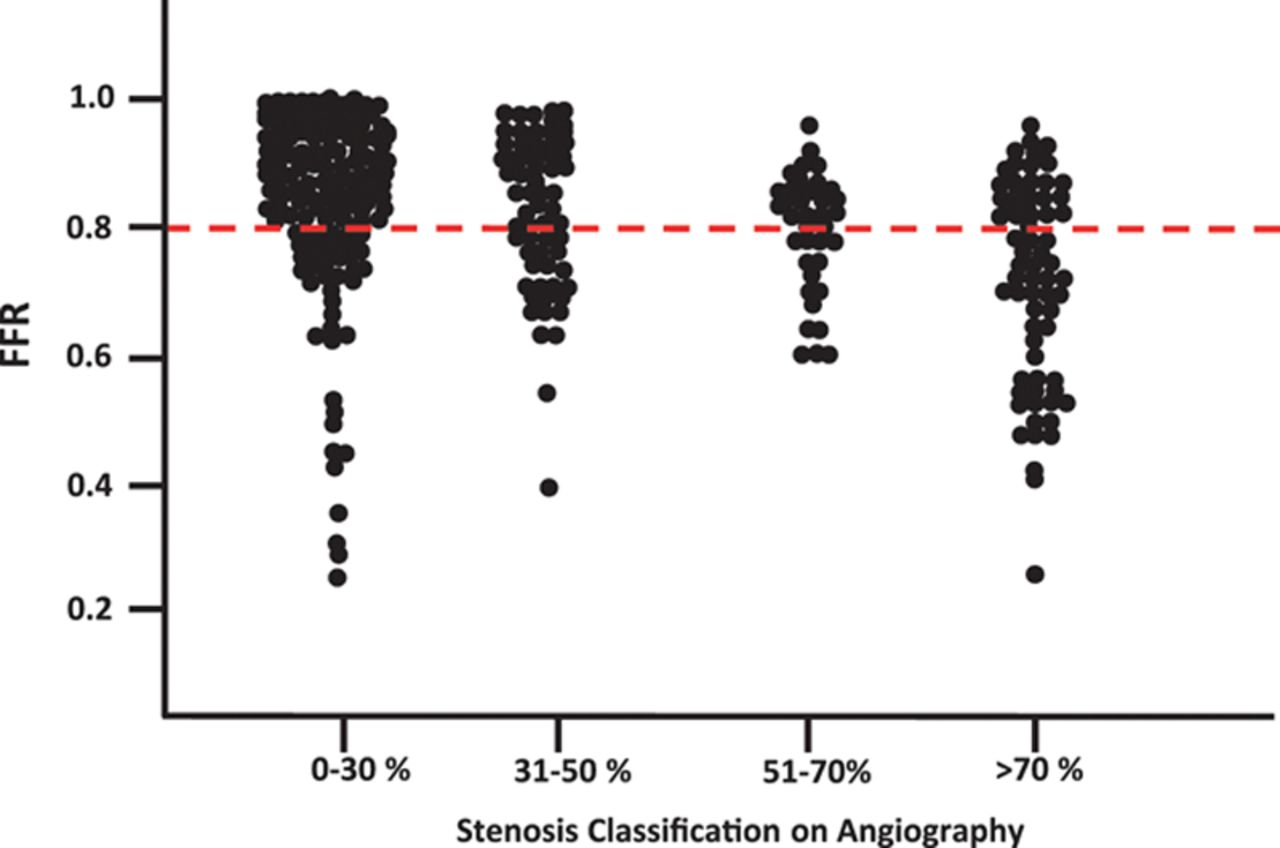
Relationship between diameter stenosis snd FFR. Note, even a 30% lesion can have a low FFR, and a 70% lesion show the FFR to scatter on either side of the cut-off value .8 . So, what does it mean? We have simply shifted our ocular bias to objective flow bias. Does Routine Pressure Wire Assessment Influence Management Strategy at Coronary Angiography for Diagnosis of Chest Pain? The RIPCORD Study Nick Curzen circulation cardiovascular Interventions 2014.
What is the effect of statin on ICL?
There is no specific large-scale study that looked into this. Plaque regression and stabilization are expected in most ICL with intensive statin regimens. (Seung-JungPark et al JACC 2016) It reduces new-onset TCFA. Will it increase the cap thickness? It can be assessed by the OCT study. (Maybe it is already available will search for it ). PCSK & Inclisiran should do it if not a statin.
Final message
Coming to the title question, the term ICL means nothing without the clinical background and the angiographic setting it is detected. Realize, the intermediate lesions don’t Imply intermediate risk. We can’t do IVUS or OCT in all intermediate lesions. Even if we detect vulnerability in a 50% lesion, treatment will remain mostly intensive medical management. (There is absolutely no good evidence to show stents stabilize vulnerable plaque that does not limit flow )
So, the best approach to all those billions of ubiquitous ICLs scattered across the human coronary landscape is to stabilize it OMT( Open-minded medical therapy), lifestyle modification (taking style out of life), reassurance, and propagation of peace that will passively the plaques. Imaging and FFR can do wonders in an elite minority population at a considerable cost. (However, for the sake of demystifying atherosclerosis we should continue research with such modalities, sparingly though )
Reference