There has been recent increase in number of women undergoing echocardiography, apparently for ruling out any hidden heart disease. In some parts of India it reached epidemic proportions that raised some concern. The folllowing post was written about this recently in this site , which evoked mixed reactions.
Now, in 2025 the new ESC guidelines for pregnancy and heart disease is released. Let us see what it says about this . Being pregnant never makes a women eligible for an echocardiogram. (No guidelines ever supported it ) It is true, cardio vascular morbidity is increasing in pregnancy as we have moved on from traditional maternal risks. May be, the new guidelines suggest we can do Echocardiography more liberally , but definitely not as routine .Please note ,it is still backed up by that mystery 1-C evidence base.
The three key words used in the guideline are
In any pregnant women
1.Unexplained cardiac symptoms
2 New cardio vascular sign
3. New cardio vascular symptom
What about women with pre-existing heart disease ?
I think, they could have included these indication in the same table. Any pregnant women with a known history of past heart disease, with or without symptoms, must undergo a detailedEcho evaluation to know the current hemodynamic status. Also, Echo should be used liberally in all in all women at high risk for cardiac morbidity (Like PIH, GDM, Obesity elderly primi, etc)
Final message
Echocardiography is simple and accurate methodology to rule out structural heart disease in pregnancy. It has great potential to detect hidden heart disease. But, it should be judiciously. Routine echocardiography to rule out a cardiac condition is becoming a non professional fad in many parts of our country What is more ironic is this practice is rampant in low and middle income countries where financial resources are scarce. It is a clearly a pathway to avoid .Let us follow the guidelines as for as possible.
Postamble
What could be the new symptom or sign in pregnancy ?
1. Mild exertional dyspnea , which was not there before . 2.A grade 1 systolic murmur across the RVOT or rumble in AV valve ? This will make every other patient (Then may be 50% of 25 million pregnancy that occur in India every year) .Still there is room to misuse the guidelines .I would argue the committee to , address the critical importance of clinical assessment and these guidelines should instill confidence to ignore physiological symptoms.
Counterpoint( Expert comment in real time from an Obstetrician)
A leading obstetrician, practicing In Chennai says she is sorry to say this. It seems many of us have lost confidence in clinical skills. In this technological era, we are unable to rely only on clinical opinion. So, echo is an easy way out. Also we are worried about legal aspects of potential miss.
I don’t know where the problem lies. In fact, one of my colleague cardiologist said , though they are confident enough to diagnose a normal heart in pregnancy by clinical means ,the referring doctor (obstetrician) often Insists an Echo.
We also know how a routine Echo might detect some innocuous entities like MVPS, a trivial TR, a dilated ventricle, a mild pericardial effusion, a small PFO, a bicuspid aortic valve, and create huge anxieties in our patients. Still… we do it to relieve ours at the cost of patients.
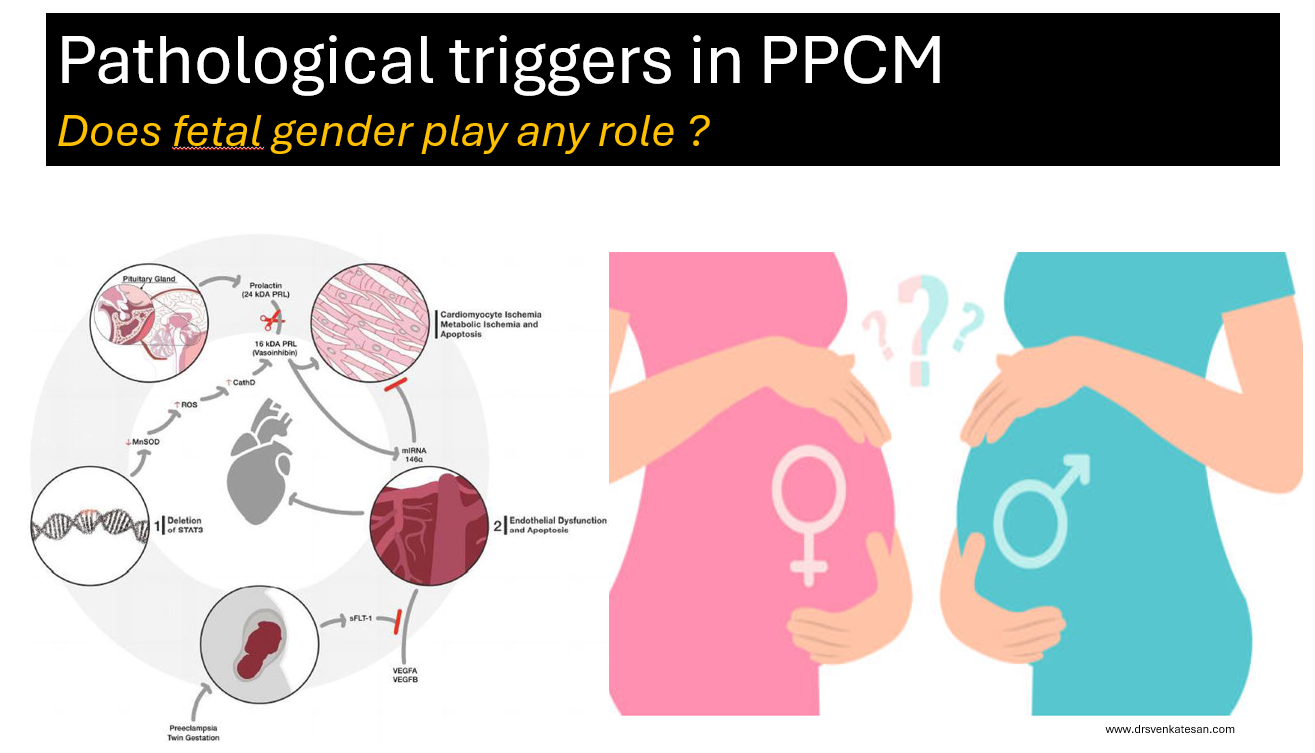
PPCM is a rare but an Important cardiac condition, that contribute to significant maternal and fetal morbidity and mortality.So many variables , triggers, back ground risks have been studied for decoding the pathogenesis of PPCM.
Does the sex of baby inside the mothers womb, in any way influence the incidence of PPCM ?
When searched in the literarure, I found almost no data on this simple parameter. While there is a lot of reference for PPCM relationships in twins and multigravida, none looked at gender specifically. From personal discussions with my Obstetrician colleagues, few suggested female babies are often seen to precipitate PPCM . I think it is an academic oversight, that we haven’t looked at the gender angle as yet, for this important entity.
Is there really no evidence ?
Yes, it is sursprisngly true . Gender as a variable may have been overlooked because it hasn’t shown up as a signal in preliminary data . Researchers often rely on patterns in existing data to guide hypotheses, and if no pattern suggests fetal gender matters, it may not be pursued. In some studies, gender data might be collected but not analyzed or reported.
It is a fertile research field. It may look like a simple study, but it can throw more light on this mystery myocardial disease that is directly related to pregnancy.
Could Fetal Gender Be Relevant in PPCM ?
While no evidence currently supports a link, there are theoretical reasons why fetal gender could be important.
Placental Differences: We know male and female fetuses have slightly different placental gene expression and responses to maternal stress, which could theoretically influence maternal cardiovascular load or immune responses.
Microchimerism: If fetal cells contribute to PPCM via immune mechanisms, sex-specific differences in cell behavior (e.g., Y-chromosome-related antigens) could be explored.( though this is speculative)
Hormonal Influence: Fetal sex might influence maternal hormonal profiles (e.g., via placental hormones), Female fetus are known to have more intense estrogenic effect in maternal circualtion.
Pregnancies with female fetuses may be associated with slightly higher levels of hCG or placental aromatase activity, which could theoretically enhance estrogen production or mimic an estrogenic effect in some contexts.(Ref 3)
What are the maternal diseases that are shown to be correlated with fetal sex ? (Ref 1, & 2)
Some maternal diseases, such as preeclampsia, gestational diabetes, preterm birth, hyperemesis gravidarum, autoimmune diseases, and asthma, have been associated with fetal gender in limited studies, with male fetuses often linked to slightly higher risks for preeclampsia and GDM, andfemale fetuses to hyperemesis and asthma exacerbations. However, these correlations are generally weak, and mechanisms are not fully understood. For PPCM, no evidence exists
Final message
Fetal gender is a simple, routinely collected variable, making it feasible to include in future studies without significant cost. If even a small association exists, it could refine risk stratification or guide mechanistic research (e.g., exploring sex-specific placental factors). The lack of data on this parameter represents a knowledge deficit in cardio obsterics that could be addressed in large registries or meta-analyses, especially as PPCM research has grown significantly in recent times.
*Request the fellows in O&G and cardiology to conduct a specific study on this topic and enrich the literature on PPCM. I think the data is already there in every PPCM paper. We just need to collate. (There is no copyright for this topic, but please acknowledge, if no one has done this aspect of a study in PPCM before)
The well known pro-coagulant state of pregnancy is an evolutionary protective process to make blood clot quicker, to save fetal loss in early pregnancy and mitigate postpartum bleeding. Still, in many women, this natural adaptive process confers an enhanced thrombotic risk. The molecular mechanisms for this pro-coagulant state are, there is increased factor VII, fibrinogen, reduced protein S. It is interesting to note, while plasminogen levels are elevated, D-dimer is also increased, indicating an ongoing fight between pro & anticoagulant forces, converting the physiological maternal- placental bed a mini harmless DIC equivalent zone.
There are several important systemic, placental, (Fetal) and cardiac indications for anticoagulants and antiplatelet agents in pregnancy. The list is increasing in a steady fashion. (Most IVF pregnancies seem to need it for some unknown reason)
Finally most importantly prosthetic heart valves & other Intra cardiac devices.
We have few options
Warfarin (Molecular weight 300 Daltons) is used in dose of 2- 10mg
Un-fractioned regular Heparin , (40000 Daltons) -Not practical for long term. Used at peripartum phase , just before labor to take control over possible PPH.
LMWH (Molecular weight 5000 Daltons)
NOACs are not an option as of now
Aspirin alone might give partial or near complete protection in some of the above mentioned indication.
General rules
Warfarin is safe for mother, Heparin is safe for fetus .(both Un-fractioned heparin & LMWH )
Just because heparin is safe, we cant choose t, it must be equally efficacious too. (Till date no study on LMWH has come to show its efficacy any where closer to Warfarin efficacy, (forget about beating it) in protecting mechanical valve events)
The concept of bridging till 12 weeks is not mandatory in all
Switching to regular heparin at term is applicable for both
Any anti-coagulant usage in pregnancy is like playing with fire .They have narrow safety window. Further, we must have have a quick antidote in case of dose excess. Warfarin, a powerful VKA, is the time tested key drug despite the well known teratogenic effect. Now we have an alternative LMWH ,which has gained considerable popularity.
The risk of Teratogenicity in warfarin is absolute or is it dose dependent ?
Yes it is dose dependent. (Warfarin causes two phases of side effects one is embryopathy, it also affects later half of pregnancy ie fetopathy with neurological bleeding etc
The Italian connect
Answer to this question came from oldest Romanian city built by the Greeks, Naples, Italy . Dr.Vitale , from the department of Cardiac Surgery, Monaldi Hospital, did this landmark study, way back in 1999 , and convincingly proved , the dreaded embryological side effects are dose dependent. It was done with a meager 58 pregnant women . The conclusions of the study changed the way we used to worry about this drug. It said, warfarin is safe at low doses even in the first trimester , if used <5mg, in terms of embryo and fetal issues. Isn’t it curious that a dreaded drug was made pregnancy friendly by simple study from smart surgeon . It is a real surprise that the conclusion of this study is still can’t be disputed by another big one. Almost all current guidelines use this 25-year-old study to form the core algorithm of current anticoagulant protocol in pregnancy.
Warfarin vs LMWH debate
Teratogen or No-teratogen, coumadin still rules supreme in most high risk situations, especially in women with mechanical valves, (Despite the ease with which this molecule crosses the placental filter , because of low molecular weight -300)
Heparin one of miraculous drug of last century , remains a life saving anticoagulant for various medical conditions. However, its refined version LMWH, though made it more palatable & user friendly, it un-apologetically took the sting out of regular heparin, made it less efficacious (more glamorous though) LMWH usage is in CAD widespread , it has suspect value* in true ongoing ischemia in any active ACS situation. It is strange anti X-a is never monitored in CAD protocol , while in pregnancy we insist on intensive monitoring i. What does it imply ? Monitoring is primarily done to ensure adequacy of anticoagulant activity , rather than risk of bleeding .
In my 30 years I am yet o see a patient have fatal bleed to poorly monitored Enoxaparin. This is the reason the mid trimester LMWH heparin bridge to collapse in many pregnancy anti-coagulant protocols. Now ,we can understand why the veteran VKAs continues to be a flag bearing drug in pregnancy .Of course, INR-guided OAC therapy, though can be tricky, most of us are used to that, unlike the frightful anti X-a troughs and peaks.
*I am sure most Interventional cardiologists will hesitate to disagree with this observation.
2022 update on LMWH : More trouble for LMWH in pregnancy. There considerable concern , that twice a day sub-cutaneous injection may not maintain target anti -X a trough .6-.8U/ml and peak 1 to 1.2 U/ml and currently many centers advice LMWH three times a day ( Bai C, Wu . Medicine (Baltimore). 2022 Dec 30;101(52):e32550.)
Final message
So far, the traditional dictum has been, Warfarin is safe for mother & heparin is safe for fetus. One has to decide accordingly with patient ,spouse & family. I think, its time to tweak this rule, little bit. Warfarin is safe for both mother & fetus* in most patients till 36 weeks in low doses , while LMWH may be more safe , but lags far behind in efficacy, especially in high risk indication. (*Including first trimester but with a lesser proof though)
Postamble
Even in these era of shared decision making, it’s our duty to impress upon our patients (or even enforce) to choose warfarin over LMWH in appropriate times. Don’t simply leave this critical decision to patients.
I think we need another study ,5, 8 and 10 Warfarin vs LMWH with a prosthetic valve and analyze the fetal bleeding risk in mechanical valves. It may not be a surprise if the cut off of 5mg could move further up.
I don’t know, whether it is a good trend, to note more and more biological vales are implanted at an young age to avoid OAC .These valves have short life span demanding redo surgeries within 10-15 years which may not be not a righteous approach.
Yesterday, my fellow informed me about a frantic call for cardiac fitness for an emergency cesarian section in 24-year-old woman with hypertrophic cardiomyopathy, who is asymptomatic and has a 20mmhg gradient across LVOT.
“Was she in labor”?
“No, she is 36 weeks term.
“Why LSCS? Why emergency”?
“I don’t know sir. Let me discuss and come again”.
HCM in pregnancy: An approach
Hypertrophic cardiomyopathy is a specific genetic disorder of myocyte (myosin and others) within the sarcomere. Though uncommon in pregnancy it raises considerable anxiety to the patient, family, and the obstetrician.
Hemodynamics
Though we tend to worry more about dynamic LVOT obstruction, it is actually the restrictive physiology of LV myocardium that might cause more concern. Three key variables operate in this entity namely preload, afterload, and contractilitythat determine the cardiac hemodynamics and possibly the symptoms. We know the classical consequence of pregnancy is a fall in systemic vascular resistance( SVR) ie afterload.
In pregnancy, there is a complex interaction between these three parameters along with heart rate. Fortunately, the net effect ends up favorable for LV performance. This is made possible because a major compensation occurs by a 50% increase in blood volume that effectively counters the deleterious effect of fall in SVR on LVOT gradient. (If mitral regurgitation is significant, the fall in SVR actually may help reduce regurgitant fraction especially if its intrinsic defect )
Maternal outcome
Is good (if not excellent). Maternal mortality reported in the literature, is gradually coming down (0 to .5%in various series) However, about 15 % of HCM patients with gross LVH or obstruction, may develop pulmonary congestion in the third trimester. In some patients, VPDs, nonsustained VT, even AF can lead to some tense cardiac consultations but are usually innocuous. I am not sure about the sudden death in pregnancy. I guess it should be negligible, unlike the non-pregnant HCM.
A mystery learning point
It is surprising both fetal and maternal outcome is little related to the severity of LVOT gradient (Ref 2)
Indication for cesarian
Most mothers can deliver per vaginalis without much hemodynamic challenge.
Vey rarely cardiac indication for LSCS need to happen. (However, in the real world many land up in LSCS , since true indication can be blurred due to cardio-obstetrical anxiety)
Spinal anesthesia to be avoided as hypotension is poorly tolerated
Beta-blockers to be continued during pregnancy labor.(Need not start however if already not taking)
Fetal outcome
Premature birth, stillbirths, low weight are little more common than normal pregnancies. Fetal bradycardia due to beta-blockers has been noted but not troublesome.
What is the role of cardiologist?
The precise answer is “minuscule role”. I can vouch for this from a personal level. ( Consults are meant only for bringing some comfort to the obstetrical team). Active cardiac interventions are rarely required or rather desired. (Of course, patients who have significant symptoms, operated for HC, on OAC for AF, the rare ones with ICD needs expert care)
Final message
Women with HCM can safely become pregnant and deliver.
Best outcome is likely for both mother, and baby if basic precautions are taken.
LSCS is rarely required*.
Counseling about the condition needs to be gentle and just adequate. Dwelling deep into the pathology, hemodynamics, and statistics in totally asymptotic patients invites trouble to all stakeholders.
*It is worthwhile to note other forms of severe LVOT obstruction like valvular, supra valvular stenosis, and Aortic pathologies like Marfan, coarctation aorta are serious entities that deserve prompt cesarian sections.
Some of the questions addressed in this presentation
1.What happens to fetal blood pressure during maternal hypotension how good is fetal autoregulation?
2.Why is LSCS increasingly preferred mode of delivery in heart disease complicating pregnancy challenging the traditional scientific concept?
3.What is likely hood of patients with moderate mitral stenosis developing pulmonary edema during prolonged 2nd stage of labor?
3.What is the missing link between PIH and PPCM? How prepartum cardiomyopathy differs from postpartum?
4.Is Eisenemneger really an absolute contraindication for pregnancy?
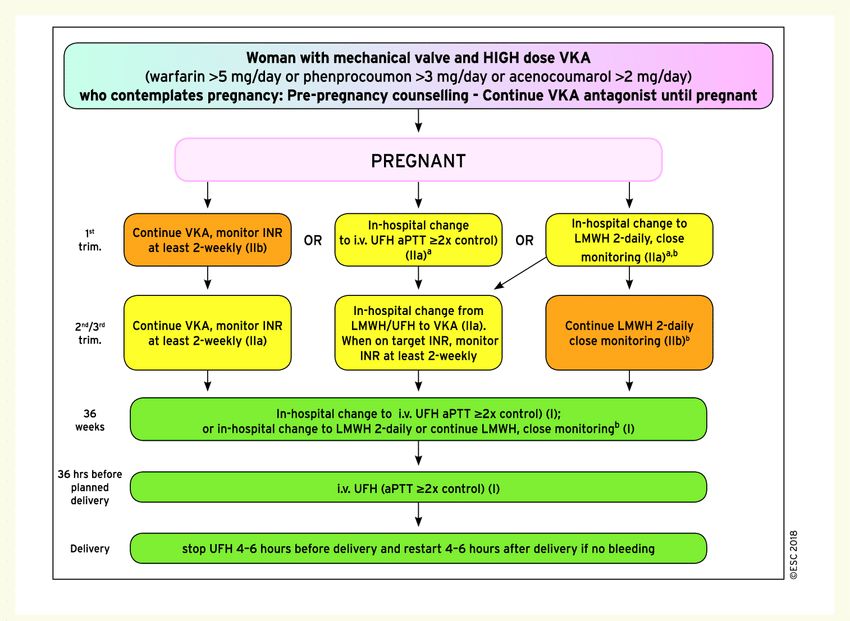
5. How can we continue VKAs warfarin or Acitrom throughout pregnancy? What are the potential problems of double switching one at 6th week from VKA to Heparin and again from heparin to VKA at 12th week?
Hope, the man-made hematological bridge in pregnancy has been finally liberated from confusion (Who is saying not yet?)
6. On what evidence base the safety margin of 5mg cutoff for Warfarin and 3mg for Acitorm was decided?
7. Who is insisting on us to do Anti-Xa monitoring for LMWH in pregnancy? Is it really needed? What does the American society of hematology say? (ASH guidelines for VTE in pregancy 2018) Why we don’t insist on Xa estimation in acute coronary syndrome?
8. What is the inflection point of at which risk of termination is almost at equipoise with continuing pregnancy in various heart diseases.
Have we ever wondered how six liters of blood in our body flows like a live stream, maintaining the fluidity life long, in spite of an active coagulation system in situ, ready to freeze at the slightest provocation (Invisible vascular wear & tear!) This housekeeping job, within the vast network of the human vascular tree, is silently accomplished by a less apparent system called fibrinolytic system. D-dimer is a physiological breakdown product of this system . D-dimer comes from fibrin monomer. The D in D-dimer stands for the domain. (See below) The ability to detect the D-dimer in the bedside has given us a good opportunity to monitor intravascular thrombus formation and subsequent dissolution in health and disease.
Formation of D-dimer from fully formed fibrin clot with the help of factor X111a and plasmin
Learning from a false alarm of pulmonary embolism
Recently I came across a pregnant woman in the third trimester with sudden onset dyspnea. Ongoing panic and a hyper response ER protocol ended up in D-dimer estimation. It was 2600μg/ml, which created a false alarm among obstetricians. She was started on heparin by then. Though her saturation was 95%, ECG was normal.An emergency bedside echo revealed normal right atrium and ventricle, no pulmonary HT. The diagnosis of PE was now rejected confidently. The much-dreaded dyspnea turned out to be some patient anxiety. Unnecessary exposure of a fragile pregnant lady to heparin was reverted with much difficulty as no one was willing to discount jacked-up D-dimer still. (Such is the power of sophisticated biomarkers and numbers! I asked them to report the elevated D-dimer as false-positive in bold letters in the case sheet and applied the break to bring the high voltage obstetrical -cardiac consult to a halt )
What is the normal D-dimer levels in blood?
In the strict sense, D- dimer can’t have normality. It is flushed-out molecular debris from clots, levles of which fluctuates depending upon the fibrinolytic load on a given day. It is further limited by lab standardization issues and methodology. (ELISA vs latex ) Currently, a level of <500μg/ml is considered diagnostically useful to rule out DVT/PVE (Good sensitivity /low specificity)
What happens to D-dimer levels in pregnancy?
D-dimer levels are nornally high in pregnancy, and can reach very high levels as well.
What is this source of D-Dimer In pregnancy?
Pregnancy is a procoagulant condition. (Estrogen Induced effect on fibrinogen and other clotting factors especially factor 2 & 7 ) We presume it is due to more microthrombus activity in materno placental capillary circulation. When there is a pro-coagulant activity, fibrinolytic activity is also high hence elevating FDP and D dimers.
Pregnancy-associated with diabetes /PIH/preeclampsia elevate it further due to subclinical endothelial dysfunction
The role of the fetus in generating or triggering maternal procoagulant activity is possible with a reverse breach in the placental maternal barrier. (Many of stillbirth, Intrauterine deaths / DIC in mother could reflect pathological faces of hypercoagulation states)
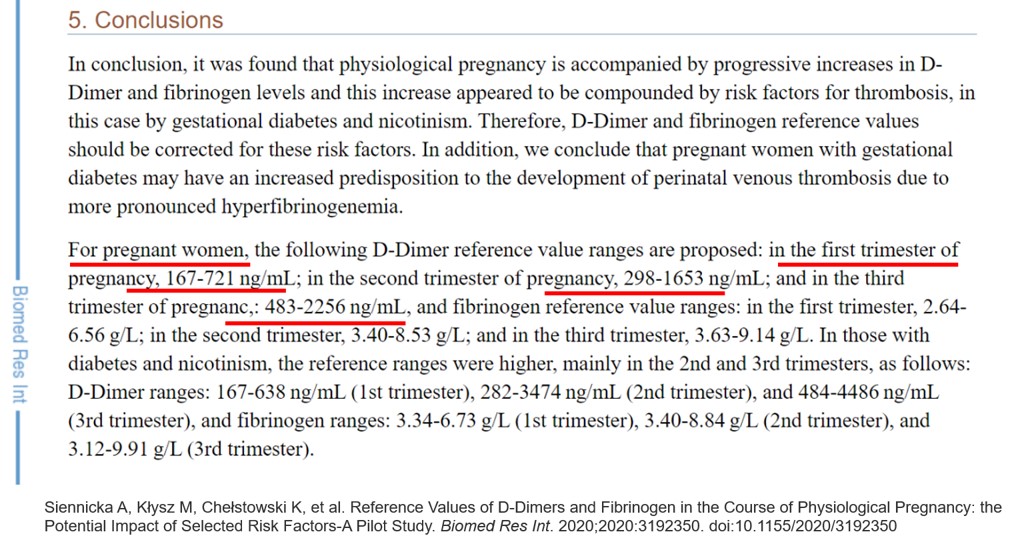
Normality redefined in pregnancy
This paper has something important. Didn’t knew this till now. In the third trimester, D-Dimer can reach up to 4400 in diabetic mothers. It is also worthwhile to note the other common causes for high D- dimers sepsis, autoimmune disorders* and occult malignancy,
*In fact, every normal pregnancy can be termed as a relative autoimmune disorder, as it is impossible for the mother to go through the pregnancy without immunological modification of the host (by fetus or host itself)
Final message
Never rely on elevated D-dimer in isolation to diagnose DVT/Pulmonary embolism. This is especially true in pregnancy where even very high levels are physiological. The commonest cause for dyspnea in pregnancy will continue to be anxiety, anemia, PIH & physical deconditioning, and weight gain (not the mitral valve stenosis /PE/or peripartum cardiomyopathy). Yes, It may appear rewarding to think like a specialist, but please realize if we diagnose rare entities, we are “rarely likely”to be correct and the consequences of that are not always pleasant.
Cardiac output in pregnancy is increased by 30 % physiologically . Hence loss of blood at the time of labor is pregnancy is sort of physiological correction .Cardiac patients do get a relief with loss of about 500 ml of blood .
Stress of Labor
Each uterine contraction is a stress to the heart and is akin to infusing 500 ml of saline into maternal circulation .This is further amplified in patients with severe mitral stenosis.
However , the maximum hemodynamic stress for the mother occurs just after delivery when about a 1 to 1.5 litre is auto transfused.One has to watch for deterioration at this point of time.
Why caeserian section is being preferred by many obstetricians in cardiac disease complicating pregnancy ?
Traditional and modern text books clearly mention , natural delivery is best for both fetus and mother in cardiovascular disease .However it is still a debatable issue in real world labor rooms, especially in obstetrical emergencies.These concepts are probably old when surgical risk were considered too high for LSCS .
My current understanding of the issue ( Subjected to correction )
Normal labor hemodynamics is unpredictable , even so in a women with critical valve obstruction
It is a “4 cornered obstetrical stress” situation , almost equally distributed between mother , fetus ,spouce and the obstetrician !
A brief period of controlled stress is better than prolonged uncertainty of labor.
Since LSCS is done in the presence of an anesthetist in a monitored and controlled setting, even a brief high risk period is acceptable till the baby is taken out.
Though technically LSCS may add a little risk to fetal life , It has been observed mothers are getting more rapid relief from post partum dyspnea who undergo LSCS.
*There is another reason for the heart to feel comfortable with LSCS in critical mitral stenosis, which threatens to precipitate acute pulmonary edema .The post partum spike in cardiac output could theoretically be less if blood loss in LSCS is accounted .(sort of venesection !)
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.