Anterior mitral leaflet has a classical M shaped motion. Infrequently , M mode echo will record a triphasic pattern .
The exact answer is not known . I guess it is a normal variant.
Often it is recorded when there is a long and redundant AML , especially if the M-mode cut is too close to the tips.
Though it is not common , I have seen in few the triphasic gets converted into classical M shaped pattern if the cursor is moved slightly away from the tip of AML.
Relationship to Heart rate
Some times it appears in slow heart rate and tends to disappear with tachycardia .
Triphasic Doppler filling vs Triphasic M-Mode
We do not know yet , how the triphasic AML motion correlate with triphasic Doppler filling pattern which is considered a fairly good evidence for LV dysfunction.
The pericarditis of acute rheumatic fever is not a true infective pericarditis.It is more of inflammation .It is primarily T cell mediated reaction . Neutrophils rarely take part in this inflammation and hence no significant exudation . Hence , there is less sticky and adhesive moleculesinside the pericardial space .The most inflamed layer is epicardium which a nothing but visceral pericardium .This layer lacks the tensile strength to constrict the underlying myocardium.
For constriction to occur the fibrinous ( thick ) layer of pericardium need to be involved . In rheumatic fever even though it is pancarditis , fibrous layer is not involved. Further the inflammatory gradient is thought to spread from within (Unlike tuberculosis )
Note : In chronic tuberculous pericarditis, diffuse inflammatory process invade from the exterior surface . Very often , one can not differentiate layers. In extreme cases even myocardium and pericardium can not be separated .
Summary
The peri-cardial effusion of acute rheumatic fever
Is transient ,non infective and resolving (Unlike valvular inflammation !)
Less of neutrophil activation (Less adhesion)
It does not involve the thick , tensile fibrous layer of pericardium hence lacks the contractile force .
Other lingering questions
1.How common is tamponade in acute rheumatic fever ?
2.How important is the mass of the effusion (Viz a Viz Intra pericardial pressure !) in causing tamponade ?
In this mean world ,most truths exist without evidence . . . and often falsehoods masquerade as truths with overwhelming evidence !
Human biology has always been a mystery and can express in dramatic ways . While , many disorders combine to play havoc on the body , few tend to protect each other. HT and DM can join a deadly coalition to attack the heart .Smoking causes extensive peripheral vascular disease , still thrombo angitis of coronary arteries ( due to smoking ) is virtually unknown. Tuberculosis does not have the courage to attack the heart valves , while it can inflict serious injuries all over the body . Similarly , systemic hypertension and Rheumatic heart disease does not combine well . So , it can be assumed some unique and hidden protective factors are at play among different pathological entities and their target organs.
A brief account of how COPD could be related to CAD ! (* Mostly Imaginary !)
We know , COPD , stresses the right ventricle by pressure overload and in extreme situation affects the LV function because of hypoxia. It rarely impacts the coronary artery disease . This has been our consistent observation. While COPD patients often land up with LV dysfunction , investigations reveal they are more of a dilated cardiomyopathy and their coronary arteries are entirely normal. Diffuse atherosclerotic CAD is a rarity in patients with history of bronchial asthma. Coronary micro circulation is also observed to be largely intact in most people with COPD .
We haven’t got a call from our pulmonology wards in many decades , for a true emergency coronary consult . Mind you ours is a 200 year old Institution , with 3000 beds , largest east of Suez canal !
It’ s very rare for bronchial asthma patients to die of a cardiac event. Thousands of elderly patients throng our ER with acute severe asthma every winter , still extremely rare to precipitate an acute coronary event !
We are yet to see critical triple vessel disease in a patients with documented bronchial asthma and COPD . Even non-critical CAD is far less frequent in COPD vis a vis general population . It is indeed a strange observation , considering both entities are rampant in the community .
What could be mechanism for the perceived disconnect between COPD and CAD ?
Is it a myth ? Does it happen in all geographical zones ? If hypoxia is the sine qua non of COPD , one would rather expect a close association with CAD , isn’t ?
One suggestion that keeps erupting from my cortex . It is the wide swinging intra thoracic pressures in COPD or asthmatic individuals . . . somehow responsible . These wide swings of pressure are transmitted to aortic root . They transform into good coronary perfusion pressure , keep the vessels clean by pressure vacuuming effect .
We have asked our epidemiological unit to analyse the 25 year data from our coronary care unit to decode the mystery .
Counterpoint
Meanwhile, a diagonally opposite question was asked in UK and found a partial proof as well . Our experience do not agree with this study conclusions .
How can a opinion (rather an Imaginary essay !) based on personal observation projected as a scientific fact ? We need to observe , analyse and publish the data . This is what the scientific world expects us to do . Unfortunately , the journey form observation into publication has been kept purposefully difficult . In my opinion bulk of the international peer reviewed medical journals with high impact factor can convert any junk data into a scientifically palatable recipe !
Platelets are humble blood cells that roam in clusters and guard against any bleeding in internal organs. Though it has natural powers to regulate itself against aggregation at inappropriate sites , certain high risk individuals need to take these drugs to prevent cardiac event. Patients who harbor intra-coronary foreign bodies like stents need more intense antiplatelet regimens.
We have variety of antiplatlet drugs. Aspirin does it by blocking COX. It is irreversible .Clopidgrel does this differently by inhibiting P2 Y12 receptors .Clopidogrel has been used extensively in India. Some brands of it are many folds costly as well !
A curious encounter
A certain patient with a stable CAD, from higher strata of society was offended when I replaced his long term prescription of Plavix(Clopidogrel) with Aspirin.His major humiliation was this new drug costs just 50 paise ! He suggested to me , it is huge insult to him as his driver also takes the same medication !
What does pride do in platelet inhibition I tried to explain him ?
He was amused !
I asked him to go elsewhere , to any star-rated , upscale health suit nearby to fulfill his wishes !
The above event happened few years ago . I am just posting it from by diary .
Final message
In this unequal world , prestige comes to play even in illness and the drugs they take ! I wonder, how prevalent, is the issue of pride in our patient’s mind that decide the treatment modality in modern day medial care !
The doctrine of modern medicine goes something like this . . .
For most medical problems , there would be a solution. Keep trying . . . till you get it !
*But , just make sure that problem on hand deserves a solution in the first place !
Modern medicine continues to remind us every day , the much hyped solutions often end up in new problems and many times worse than the original problem !
Oh ! what a great a quote ! When I was boasting myself . . . My wife reminded me , this is just plagiarized version of a 2000 year old Hippocratic thought !
Inter atrial septal aneurysm is a benign disorder of IAS where the flap of fossa ovalis bulges on either to right or left atrium. It may be associated with fine fenestration or even a classical ostium secundum ASD.
An unusual buckling motion of IAS aneurysm.
Though the pressure within the atria is one of the determinant of this bulge.The morphology of the flap is such that it more often prolapse into LA than RA. Rarely it can be dynamic and moves 180 degrees , buckling between RA and LA .This unusual motion is real stress to IAS and can trigger atrial ectopic beats. and atrial tachycardia .
Human physiology can dramatically surprise us.Here is a situation regarding K+ ion and cardiac function.
Low potassium level is a well known cause for skeletal muscle weakness and paralysis.While,in cardiac muscle usually the opposite happens.It is the high potassium levels that depresses and cause paralysis.(That’s why,it is used in cardioplegic solutions. )
But,the classical differences between skeletal and cardiac muscle need not apply in critically low levels of K +
What happens when K + is critically low ?
We know, K + is the vital ion that maintain not only the membrane potential ,(Recall Nernst potential ) but also keeps the action potential floating and dipping with every beat.
Imagine the intracellular chaos when these ion levels changes in dramatic fashion . (Of course,God has ensured very tight regulatory controls at various levels within each cell ! )
However , ECG changes are expected 100 % of time with falling K + especially below 3meq.Surprisingly , low K + levels have little mechanical impact.(Or is it our ignorance,considering the fact , cardiac electrical mechanical activities are tightly coupled?)We have to find answer from patients like this .
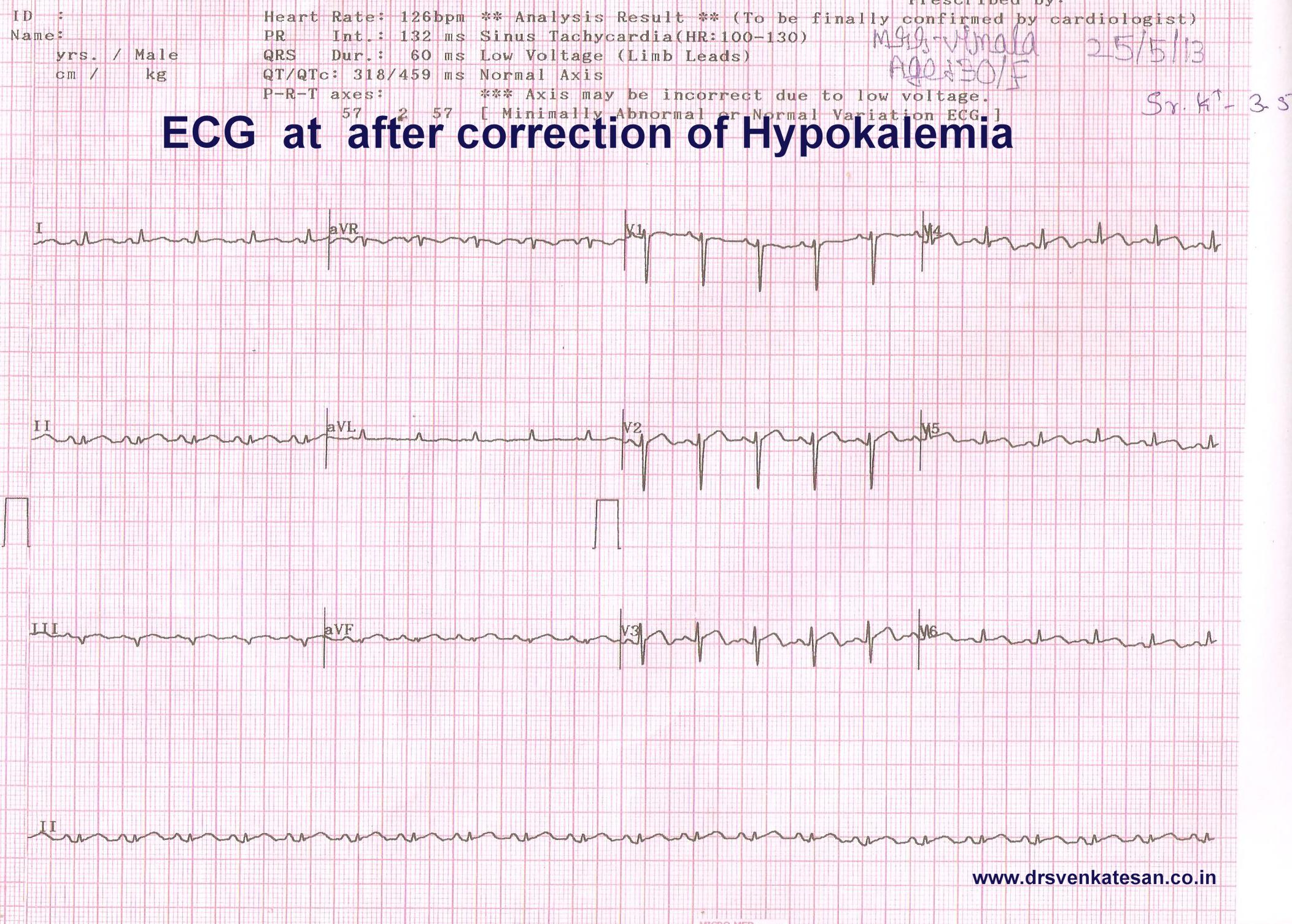
A 30 year old women came with breathlessness and fatigue and her ECG.
Can we afford to miss a diagnosis of STEMI ? With all our collective wisdom STEMI was diagnosed promptly . . . of course wrongly !
She was adviced streptokinase.A shrewd fellow who reviewed the old records spotted the past history hypokalemia , and Inj streptokinase was put on hold.(Lucky patient . . . she was not shifted to cath lab )
Her K + was 2.3 Meq. The LV function was significantly impaired with global hypokinesia, which improved with correction of K+.
She was later referred for nephrology work up , they had made a possible renal tubular disorder for the Hypokalemia.
Clinical Implication.
When potassium levels are critically low myocardial function may deteriorate.Here is a patient with dramatic STEMI like ECG with extreme hypokalemia.
Our ignorance regarding electrolytes and myocardial function remains unexposed .In critical care units wide swinging metabolic and electrolytic parameters are common.ECG is just a marker for these .Similarly all LV dysfunctions are not primary myocardial disorders (Sepsis, Hypoxia, Extreme acidois , Uremia ,drugs,toxin can lead to myocardial dysfunction.)
Experienced physicians do not form hurried opinion.Wait . . . allow things to settle down and assess again.After all ,there is long list of causes for ST elevation other than STEMI !
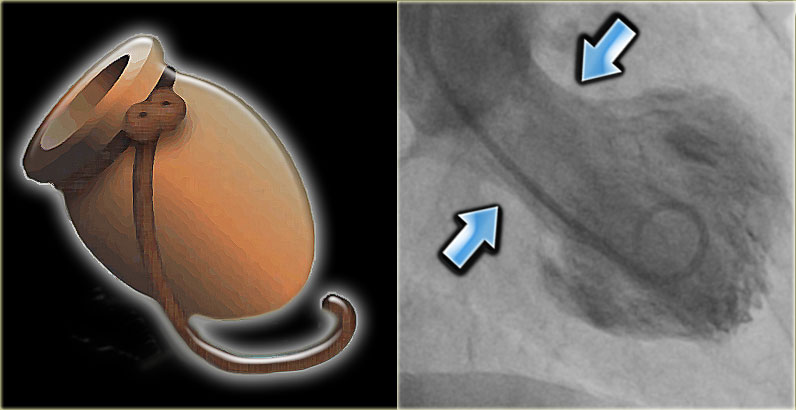
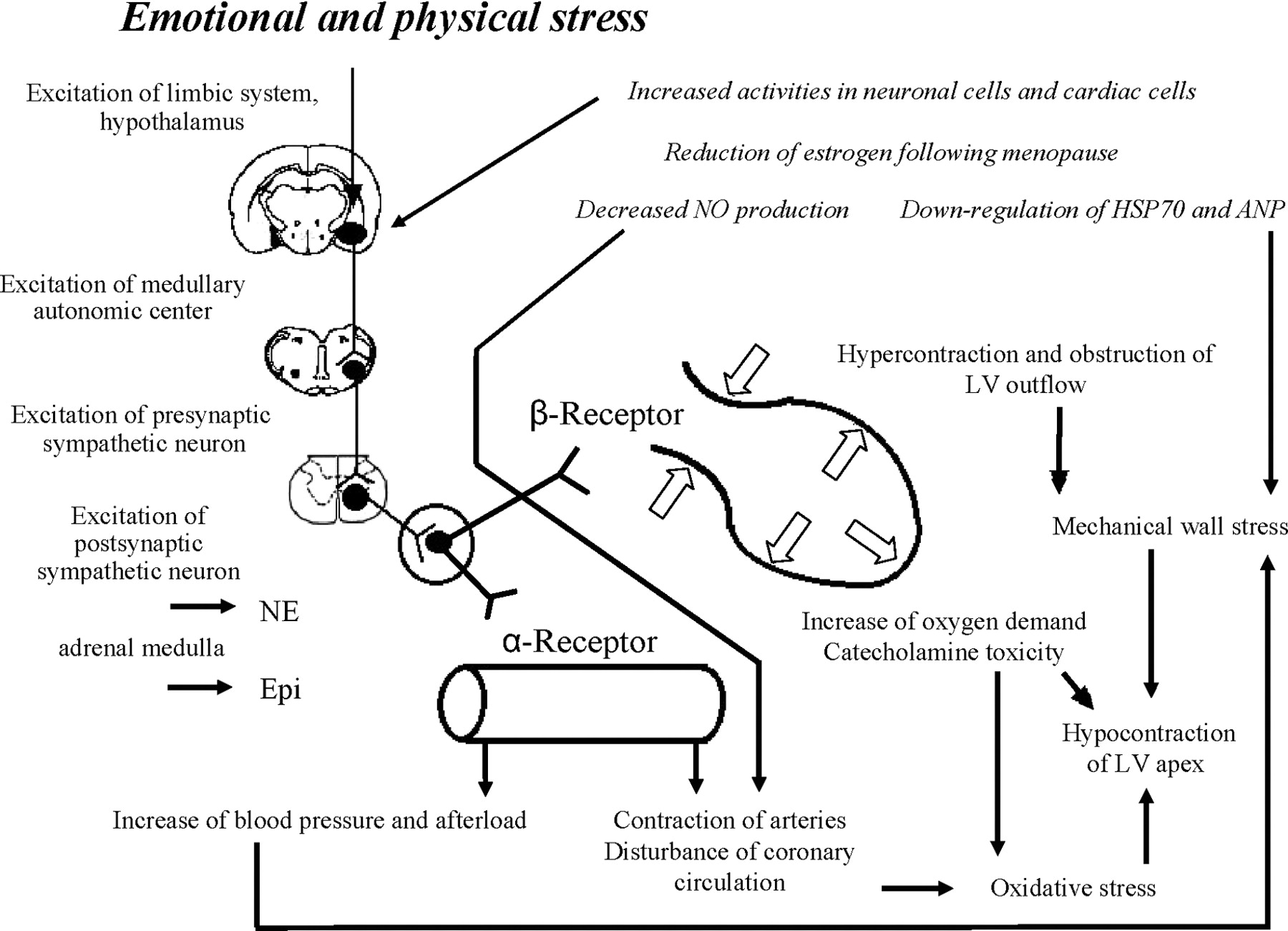
Takotsubo cardiomyopathy is an unusual response of the left ventricle to extreme emotional stress .The catecholamine surge has a profound stunning effect of LV apex and a paradoxical hypercontractility of basal LV.
The exact mechanism is not clear , Following factors may contribute.
Multi-vessel coronary artery spasm,
Cardiac microvascular dysfunction.
Abnormal myocardial fatty acid metabolism,
Reperfusion injury after an ACS *
However , the most accepted mechanism is Endogenous catecholamine-induced myocardial stunning and microinfarction
The adrenergic receptor distribution is high in LV apex .They are exposed to high concentration and gets stunned easily . Basal LV has less adrenergic innervation , so it shows less of catecholamine toxicity , instead it exhibits. hyper-contractile mode. However, this rule is not absolute.
One more suggestion was apical balloons correlated with wrap around LAD.(Báñez B et all 2004)
1.Báñez B, Navarro F, Farré J et al. (2004). Tako-tsubo syndrome associated with a long course of the left anterior descending coronary artery along the apical diaphragmatic surface of the left ventricle.]”. Revista española de cardiología (in Spanish; Castilian) 57 (3): 209–16
Scientific studies can be fun .In our spare time we often Indulge in rapid fire sessions. We tested 30 wide qrs ECGs from our archives (All proven VTs) and asked our cardiology fellows to apply Brugada criteria . They could correctly diagnose VT in 18* patients.The same ECGs were shown to the staff nurses of coronary care unit . 24 VTs were correctly identified it.They did it by their clinical sense and Instinct. (*12 vs 6 VTs missed)
And now , four clinical data was provided. (Age , sex , Blood pressure , and past H/o MI were given ) The Nurses were able to predict it 28/30 VTs correctly.(97 % accuracy ) and the cardiologists were able to equal the score now. So obviously clinical sense was far superior .
Cardiology fellows were more likely to mistake VT as SVT. This is far more common than SVT mistaken as VT. It is a strange academic irony ,even the junior most nurses never missed a VT !
Summary
Simple sequence of history and clinical presentation is still far more powerful than ECG data in predicting wide qrs arrhythmias . Nurses guess work is far superior than cardiologists in predicting a wide QRS tachycardia as VT.
In fact , the cardiology fellows are preconditioned to get confused whenever they get a wide qrs tachycardia . Why not aberrancy ? In my experience I have seen this question keeps erupting inappropriately .Even shrewd fellows suffer from an oscillatory mind between VT and SVT .This is primarily because , every wide qrs ECG is likely to have at least two criteria that fulfill both VT and SVT.
The implications are genuine and far reaching . While nurses show a patient centric thinking cardiology fellows thought process revolves around ECG . Many modern-day cardiac physicians are disconnected from clinical reality and are obsessed with complex EP concepts and end up with a miserable face in the bed side !
This is not a new revelation in 2013 . Masood Akthar told this three decades ago.
Caution
Never try to glorify guess-work . EP is a great science .The pioneering concepts have made us understand how a VT emanates, travels , and exit from myocardium . We are able to localise it and ablate it .All credit goes to science . But , when it comes to bedside recognition of VT , clinical sense is a clear winner .With a consistently > 90 % predictive value it can no longer be called as a guesswork and becomes a hard scientific fact. Especially so , when the intellectual analysis of surface ECG could predict it with paltry 70 % accuracy (Read Reference 1)
This analysis startlingly reveal a fact .The over all accuracy rate of predicting the wide qrs criteria by popular algorithms is between 66-77% , just 16 numerals more than gross guess work of 50 : 50 ( This . . . or . . . that )
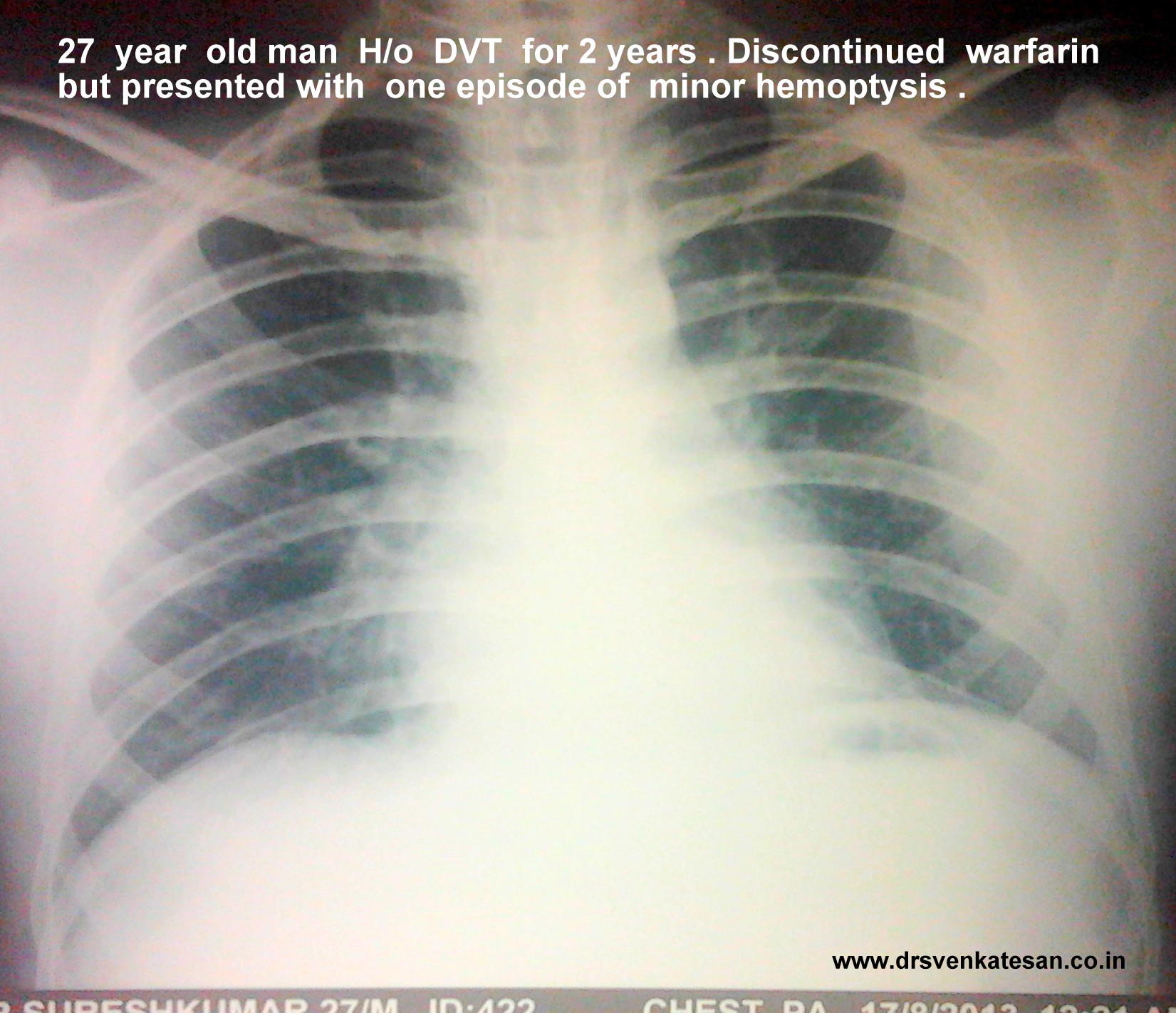
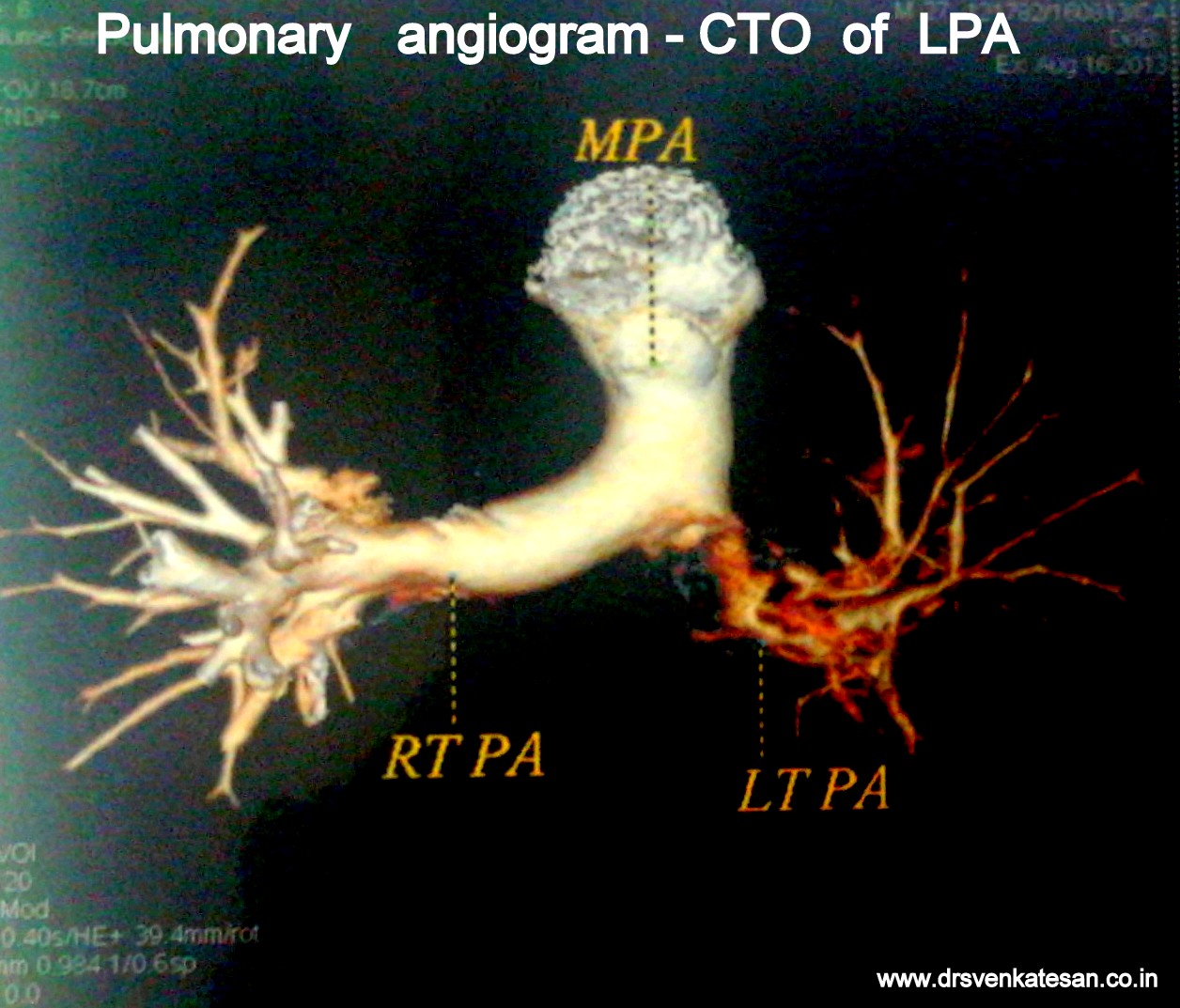
A 25 year man , hotel manager who had a documented DVT , since 2011 was on tablet warfarin . He discontinued the drug by sheer miscommunication as he was told he should stop the drug beyond INR 3 by his general practitioner.He stopped it permanently instead of titrating the dose of warfain .Six months later he landed in August 2013 with an episode of minor hemoptysis . Clincally he was normal .His lower limbs were fine.
He was investigated and his image file showed .
Living with one lung
He is comfortable with one lung function (Akin to Pneumonectomy )
His saturation was 100 % at room air
Pulse -80/mt .BP 110/80mmhg
His physical activity did not show any significant limitation (At worst class 2)
One of the cardiac surgery consultant wanted to do pulmonary embolectomy and endarteriectomy .
In fact , he was admitted in the critical care unit driven by the dramatic CT images.
One enthusiastic cardiologist wanted thrombus aspiration and pig tail catheter based thrombolytic irrigation within LPA !
How did we manage ?
The risk of major vascular surgery was considered high in an absolutely asymptomatic individual .
Intervention was considered too adventurous.
He was put on oral anticoagulant with target INR 2.5-3.(After a 1 week Heparin overlap)
We hope the thrombotic CTO will open up gradually but for surely .As the power of natural lytic molecules should not be underestimated as we have witnessed in LV and LA clot disappearing over months.
However the option of putting IVC filter was strongly recommended for him , as he has only functioning lung which is threatened by a potential embolus from DVT . The patient wanted to come back for IVC filter next month.
He was also worked up for all those protein C, S, Lieden mutation stuff.
The patient was discharged in stable condition (By the way he was never unstable either !)
* Meanwhile the hemoptysis did not recur. CT scan showed a small wedge infarct in left lung that was in the healing mode.
Final message
This is a perfect example of CTO of pulmonary artery being managed conservatively* .We will let you know the follow up .
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.