Current data from TCT
TCTMD – The Source for Interventional Cardiovascular News and Education
Posted in Cardiology-Coronary artery disese, tagged tctprimarypciexportcatheter on September 25, 2009| Leave a Comment »
Current data from TCT
TCTMD – The Source for Interventional Cardiovascular News and Education
Posted in Uncategorized, tagged BARI 2D, chronci stable angina, courage study, csa, drsvenkatesan, ethics in cardiology, journal of clinical cardiology, oat study, pci vs cabg vs medcial on September 25, 2009| Leave a Comment »
Medical profession has evolved over centuries with humble discoveries by genuine researchers in the past . As we pursued science vigorously , we looked for innovations , when innovation work ( or many times shown to work !) we jump to sky , even as some of these innovations fail and crash down to earth , many times we continue to be in the clouds . This is the fundamental problem of modern medical science . When our expectations reached unrealistic proportions , we tend to lose the common sense . Prolonging life and reducing human suffering may be the ultimate aim of the medical profession , but If we try to fight the death with science and money without application of mind , our current life may become miserable ! Thats what is happening for the majority of the population of this planet . After all , death is an essential and final component of life !
Coming to the issue of CAD , in our country , a rich gets a 4th generation drug eluting stent for a insignificant asymptomatic PDA lesion , and poor fellow with left main dies without any intervention .This is fairly acceptable to this uneven world , where a rich westerner dies due to obesity related disease and a poor African dies to malnutrition .
This article is in response to my recent experience when . . . I advised
Simple life style modification & few drugs for a patient with chronic multivessel CAD , I was made to look ordinary , inferior and funny by many of the current generation cardiologists .
Further , the term optimal medical therapy(OMT) for chronic stable angina has evoked laughter in one of the interventional cardiology conferences I attended !
It is a sorry state of affairs for the whole cardiology community , a genuine scientific fact , proven by real life experience as well, is being ridiculed.
Richard Conti tells in this excellent editorial in his journal Clinical cardiology about the issue of medical management of CAD
“Respect in clinical trials”

Click here to reach the article http://www3.interscience.wiley.com/cgi-bin/fulltext/122512853/PDFSTART
A similar study which suggested exercise could be better than PCI in the recent 2009 ESC is suffering the same fate !
What if regular exercise were as good as a stent for stable angina?
Posted in Uncategorized, tagged great cardiology web site, great medcial videos, great medical web site, innovations in medical education, top medical sites, university of wisconsin on September 23, 2009| Leave a Comment »
Internet has revolutionised in sharing our knowledge . But , the freedom it gives has a trade off .Identifying genuine knowledge in the vast cyberspace is like searching for lost treasure in the ocean bed.
Have a look at this site which innovates medical teaching

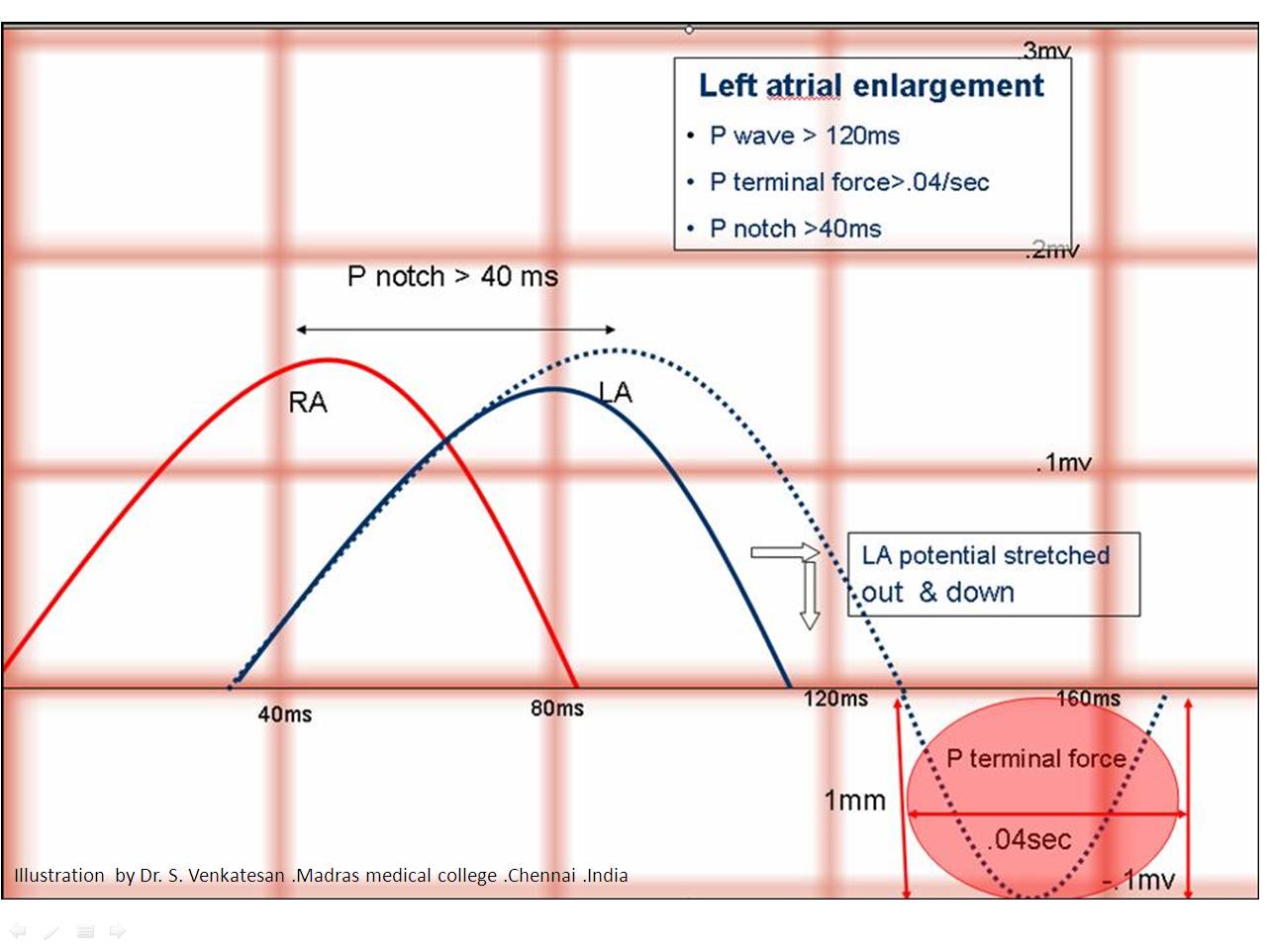
Posted in Cardiology - Clinical, cardiology -ECG, Infrequently asked questions in cardiology (iFAQs), tagged bi atrial enlargement, can p wave be tall in lae ?, how LAE widens p wave, how to diagnose left atrial enlargement in ecg ?, LAE, left atrial enlargement, NOTCHED P WAVE IN LAE, P PULMONALE, p wave abnormality in ecg, p wave in ecg, RA vs LA depolarisation, RAE, Right atrial enlargement, why p wave is tall in RAE and wide in LAE ?, why p wave is wide in lae ? on September 20, 2009| Leave a Comment »
Normal P waves

What are the components of Pwave ?
RA component : The SA node depolarises the RA first , so the initial part of P wave represents RA current .After about 40msec the wave front reaches LA and it begins it’s depolarisation .LA component :By the time LA is maximally depolarised the RA already starts its repolarisation.So there is overlap and also a short time lag between these two wave forms . This is very important to recognise as , even if the RA conduction is prolonged in pathology the RA component of P Wave still falls within the LA wave .Hence it is not shown in the ECG and P wave is not widened in RA enlargement. This is in contrast to LA enlargement , when the terminal half of P vector delayed it stretches the P wave wide beyond the normal 110ms .Hence LAE widens the Pwave.
Why P wave becomes taller in RA enlargement ?
In classical P pulmonale , the P waves are tall >2.5mm. It is easy to explain why it not getting wide than why it is getting taller ! The atrial vector has two components .The initial RA vector is directed anteriorly .The main reason for tall p with RAE is due to the anatomical proximity of RA to the chest wall Further ,the Initial atrial electrical dp/dt is steep . Any RA voltage increase is easily picked up by the chest leads and P wave voltage increase and becomes tall. We need to realise LA is not only left of RA its equally posterior of RA. Hence LA enlargement rarely brings (Never ?) it closer to chest wall ,and hence high voltage tall P is almost unheard of with LA . Note , deep negative late P wave activity is typical of LAE , consistent with its posterior location as well its late depolarisation compared to RA)

Why LAE can not produce tall P wave ?
The Left atrial vector which follows RA vector is mainly directed posteriorly and hence inscribe a descending limb of P wave . This causes the P terminal force . So the direction of vector forces and the anatomical locality make a tall & positive P deflection highly improbable in LAE .
*Of course when LAE is huge , where a antero -supero vector from roof of LA may inscribe a positive wave .
What happens in bi atrial enlargement ?
It can have features of both . Tall & wide P waves .
Can RA generate a Q wave ?
Yes . When RA assumes a huge size , especially if the RV is also at high pressure as in severe PHT or valvular PS a q wave is generated in the lead V1 .This q wave is nothing but the intra cavitary potential of the enlarged RA.
What is the difference between atrial enlargement, atrial dilatation, atrial hypertrophy, intra atrial block and inter atrial block ?
The p wave morphology has no specificity to identify the various entities. In any pathology of atrium the first thing that happens is a conduction delay ! It is now realised the bulk of the changes we see in atrial enlargement especially in LAE is due to intra and inter atrial blocks or more subtly conduction delay.
It is obvious , a wide P wave can occur either due to LAE or simple conduction delay .In elderly hypertensive patients atrial fibrosis is more common , one can not confirm LAE without echocardiogram .
A notched P wave can be a very specific sign of inter atrial block .Which is more common in severely diseased left atrium. A notch , slurred p wave is a good marker for impending AF or atrial flutter.
//
Posted in Uncategorized, tagged bio ethics, mechanism of drug action, pharma industry, pharmacology on September 19, 2009| Leave a Comment »
Pharmacology is a major discipline in medicine where we learn how a drug acts in our body for various ailments . Now in this era , doctors need not only how a drug acts but also how a drug company acts ! This has become vitally important for the welfare of the mankind .
In this context one of the best books on medical pharmacology is from the
Famous Editor of New England journal of medicine
A must read for all genuine medical professionals

Watch Marcia Angell talk http://www.youtube.com/watch?v=ouF3ISihHLM
Full lecture of Mercia Angell http://videos.med.wisc.edu/videoInfo.php?videoid=940
Click to buy/read the book http://www.amazon.com/Truth-About-Drug-Companies-Deceive/dp/0375508465#reader
A Review about the book http://calitreview.com/176
Posted in Uncategorized, tagged avnrt, brugada criteria, ECG, ep study, infectious disease, pace journal, podrid, supraventricualr tachycardia with aberrancy, svt, svt vs vt, ventricular tachycardia, vt vs avnrt, vt vs svt, what is wide qrs tachycardia, wide qrs tachycardia, width of qrs, zipes on September 18, 2009| 1 Comment »
Wide qrs tachycardia has a unique place in clinical electrocardiography .It is a much fancied and glamorous entity for the simple reason , it continues to be the cardiologist ever solved puzzle .For over three decades of research, clinical debates , symposiums , seminars have effectively failed to take away the uncertainties in decoding the wide QRS tachycardia . (Specifically , VT vs SVT with aberrancy)
Some wondered , should we really waste our efforts in differentiating the two . In emergencies it never matters , in fact one need not attempt to do this often futile exercise !
Few dedicated criterias like Brugada etc have helped us .
While the difficulties in differentiating between VT and SVT with aberrancy remain over the decades .A less reported , but more common issue is confronting us .
It is the big question of differentiating a wide QRS tachycardia from a narrow QRS tachycardia
This occurs more often than we realise ,because we define wide QRS tachycardia in a vague manner
* The confusion is mainly because 20ms difference between limb leads and chest leads .
In reality one may not be able to all tachycardia into narrow or wide .
There is big overlap zone that need to be labeled a intermediate qrs tachycardia
If we can triage the tachycardias into three instead of two it may help us arrive fast , to the correct diagnosis
Narrow QRS tachycardia ( qrs 80ms)
Intermediate QRS tachycardia 90-120
* Any VT that arise near the major conducting system of ventricle conduct fast and hence qrs are relatively narrow.
**These are rare entities where base line wide QRS getting narrower with the onset of VT . (Ref : http://europace.oxfordjournals.org/cgi/content/full/eun254v1)
Wide qrs tachycardia >120ms
Unresolved questions
Final message
When we are able to solve complex electrophysiological problems , we must also realise even simple tasks can be demanding in medicne ! It is proposed to create a new group “Intermediate QRS tachycardia “that can help solve the issue where we have difficulty in labeling these tachycardias which fall in the greyzone .We can try & apply the modern EP based VT criterias to this group and find out the hidden truths !
Posted in cardiology -ECG on September 17, 2009| 3 Comments »
The most popular criteria to differentiate VT from SVT aberrancy is formulated by Brugada in 1991.
The greatness of this criteria is that a single question asked is able to confirm VT in vast majority of cases.
Is RS complex absent all of the pericardial leads ? If the answer is yes it is VT 100%
How is that, we have been struggling for so long , a single question is able to solve the issue quite easily ?

This is because , the term “Absent RS complex ” actually means
Presence of one of the following three typical complexes Of VT.
Two of them actually imply , q waves throughout V 1-V6 .This means a badly damaged ventricle and with little electrical activity coming towards the chest wall .This situation almost always occur in VT.*
The third complex is Monophasic R .
A monophasic , wide QRS complex again indicate VT as monophasic aberrancy is very rare as the supraventricular impulse invariably conducts with RSr’ (The right bundle refractory period sees to that at least a small r’ is inscribed however fast the SVT is ! )
So if there is no RS complex it must be VT !
What are the difficulties faced in applying this first step of Brugada criteria ?
It is funny to note , in medicine criterias often work perfectly in text books only !
Is there a RS complex seems to be a very easy question ? There lies the catch ! .Even though this criteria may be 100% specific , differentiating RS from QS complex even by an experienced cardiologist may be difficult in a significant number of VT tracings.This realistically , reduces supposedly 100% specificity of this criteria !
In fact we expect Brugada to develop an another limb to his now famous algorithm
Is there absence RS complex in precardial leads ? Yes / No / May be , not sure !
Posted in Uncategorized on September 15, 2009| 7 Comments »
Left main disease is an important subset of CAD , and it has special interest for the interventionist. Traditionally cardiologist have a fear to touch this lesion , as they thought a sudden occlusion within this vessel is life threatening . Later on as they gained experience it was thought we could intervene safely at least in protected left main . Subsequently it was realised this fear was largely unfounded , after all the proximal LAD is equally dangerous and we spend hours together inside an LAD ! .Now we have technology and expertise to do successful PCI any where in LM. And unfortunately , the same expertise is not applied in selecting the ideal patients who will benefit the most . LMD has become a glorified indication for PCI.
The terminology of protected and unprotected LMD is in vogue for many years . Unfortunately it do not convey a uniform meaning . In next few minutes , I shall share my views on the nuances of protected and unprotected LMD .
The term protected was not coined by cardiovascular physiologists but by interventional cardiologists . Hence it connotes a anatomical meaning rather than physiological. Protected LMD meant there must be a at least one graft to either LAD or circumflex . And this graft should be functional . The presence of this graft is supposed to increase the comfort levels of the interventionist as well as the patient.
A left main coronary artery disease angiographically can be classified as
Common types of Left main lesion
Unprotected left main
Protected left main
Partially protected Leftmain
It could mean any of the following, Left main Plus . . .
The above 3 situations may demand a PCI .But logic would suggest one would try to open up the partially occluded graft rather than open the left main . Of course the decision involves status of RCA .
*The only indication for a PCI in protected LMD could be 4
Can left main be protected by collateral circulation ?
It is very common to find Left main bifurcation lesion with LAD having very good collaterals from RCA sometimes filling up to proximal LAD .This can be considered “protected left main equivalent”
As on today , cardiologists would rather believe a surgeon’s graft rather than a naturally grown collateral from RCA however extensive it may be !
But logics and real case experience would indicate in a patient with LMD and an extensively collateralised LAD can in fact be considered a protected left main.
If a left main is well protected by a functional LAD graft , why should we do a PCI for left main at all ?
This question was risen in one of our cath conferences , a patient who had functioning LIMA to LAD graft.His RCA had a functioning venous graft and his circumflex had a partially functioning graft.The left main had a near total obstruction and the proximal LAD was faintly visible .
Since the patient had class 2 angina Options were discussed .He satisfied the current criteria of protected LMD .Just because he fulfils the criteria of protected left main , he does not become eligible for left main PCI . After all he is having this LMD for many years. Protecting again the left main which is already protected is not a big deal in terms of outcome . Double protection is waste of resource at additional risk. It was decided to attempt a PCI to SVG graft to LCX. If it does n’t work leave him with medical management.
Does every patient after a CABG has a high chances of developing LMD ?
What is accelerated atherosclerosis of Left main following LAD /LCX grafts ? It is true left main has high risk of accelerated atherosclerosis and it undergoes gradual obstruction once the LAD and LCX is grafted.This is due to low flow across the native left main as distal grafts maintain the flow . This is all the more likely in good bulk of patients who had undergone CABG where LMD was the indication .
A typical scenario
A left main patient who undergoes a CABG a follow up for a suspected angina angio after 5 years show the totally or near totally occluded native left main . Sudden Visualisation of worsened leftmain disease makes this patient eligible for a PCI as he fulfills the criteria for protected leftmain .
Final message
A well protected left main with a good functioning graft especially to LAD most often do not require a fresh revascularisation procedure irrespective of the tightness of left main disease . Most of such patients will be candidates for medical therapy .Contrary to the popular belief , left main intervention could be confined to ” unprotected LMD rather than well protected LMD” as the potential benefits are more .Further interventional resources need not be wasted in giving second alternate protective channel for an already protected vessel !
Of course it should be remembered in any given patient with protected or unprotected LMD the indication for revascualrisation is based on the severity of lesion , symptoms, LV function , residual ischemia, viability etc .
Suggestions , comments and corrections welcome
Posted in Cardiology - Clinical, cardiology -ECG, Cardiology-Arrhythmias, tagged av dissociation, av dissociation by usurpation, avd, capture beats, chb, complete heart block, drug induced av block, fusion beats, interference av dissociation, pathological av block, physiological av block, reversible av block, transient av block, va association, va block on September 13, 2009| 3 Comments »
CHB and AV dissociation are often confused with one another . While CHB is an important cause for AVD , there are distinct differences which have clinical implications. This table is an attempt to simpify the understanding of the two. Corections and suggestions welcome.
This is a high resolution image , to read better right click on the table copy image and open in any image viewer
Posted in Cardiology - Electrophysiology -Pacemaker, Uncategorized, tagged cardiac resynchronisation therapy, care chf, companion, CRT, madit chf on September 12, 2009| Leave a Comment »
Atrial fibrillation and CHF are close companions. Either it precipitates CHF or follows it.In advanced heart failure of any etiology the incidence of AF can be up to 40% .Medical therapy of AF is fairly effective in patients with normal LV function .But when associated with refractory cardiac failure it becomes too complex to control .
Currently CRT with ICD is becoming the standard OF care for advanced CHF. The efficacy of CRT is being rigorously being assessed . Even as the controversy about the wideness of QRS is being settled , the issue of optimal timing of CRT has risen . Now , the MADIT-CRT has answered this issue “Earlier it is better , it can be indicated even for class 1 patients”
While MADIT -CRT will increase the number of CRT implants , we have no clear cut answer for the efficacy of CRT in patients with AF .( Of course , the MUSTIC and CARE HF sub group analysis suggested AF has no significant impact on CRT efficacy )

Why is AF important in CRT ?
There are two issues that need analysis
Impact of AF during CRT
Presence of AF at the time of CRT gives us an opportunity to tackle this issue.
How to tackle sudden AF induced CRT response ?
There are variety of algorithms available to
In dual chamber pacing mode switching converts DDD into VVI .This happens at the cost of loss of AV synchrony .This may have profound implication in CRT .
Then the big question comes . What is the use of having Intraventricular and interventricular synchrony without AV synchrony ?
When nothing works .The best strategy is ( Rather deemed to be best ! )
Note : Ablation of AV node and putting a dual chamber pacing can never guarantee a physiological pacing as the atrium continues to fibrillate and AV synchrony is rarely there .
Final message
For CRT is to be successful , there should be maximal Bi-Vi capturing , of course this capture has to optimally timed , and must reverse the three pathological asynchronies , namely intraventricular , Interventricular and atrio ventricular asynchronies.
It is obvious , presence of AF complicates the issue as it demands constant monitoring and programming of the device (Of course now most of them are automated) . It may require knocking down of AV node , which not only carries a risk of SCD * , it also make these patients permanently dependent on the RV pacing . This adds on , another risk , for an acute complication if the RV lead fails for some reason.
Reference :
EP experts generally take too much liberty in adopting this strategy for the simple reason it solves the nuisance of atrial impulses interfering with ventricular leads function that result in inappropriate ventricular capture fusion or ultimately poor BiVi pacing . But it is not an easy decision atleast for the patient ! This article , emphasises the dangers involved in ablate and pace strategy for uncontrolled AF.
Further reading





