Wide qrs tachycardia has a unique place in clinical electrocardiography .It is a much fancied and glamorous entity for the simple reason , it continues to be the cardiologist ever solved puzzle .For over three decades of research, clinical debates , symposiums , seminars have effectively failed to take away the uncertainties in decoding the wide QRS tachycardia . (Specifically , VT vs SVT with aberrancy)
Some wondered , should we really waste our efforts in differentiating the two . In emergencies it never matters , in fact one need not attempt to do this often futile exercise !
Few dedicated criterias like Brugada etc have helped us .
While the difficulties in differentiating between VT and SVT with aberrancy remain over the decades .A less reported , but more common issue is confronting us .
It is the big question of differentiating a wide QRS tachycardia from a narrow QRS tachycardia

This occurs more often than we realise ,because we define wide QRS tachycardia in a vague manner
- Normal qrs width between Up to 80 / up to 100 ms acceptable ?*
- Narrow qrs tachycardia 80 ms?
- Wide qrs tachycardia i> 120ms ?
- Definitely wide qrs >140msec
* The confusion is mainly because 20ms difference between limb leads and chest leads .
In reality one may not be able to all tachycardia into narrow or wide .
There is big overlap zone that need to be labeled a intermediate qrs tachycardia
If we can triage the tachycardias into three instead of two it may help us arrive fast , to the correct diagnosis
Narrow QRS tachycardia ( qrs 80ms)
- Sinus
- All svtS (avnrt etc)
Intermediate QRS tachycardia 90-120
- Most of the SVT with aberrancy ( Except antidromic SVTs which are really to wide !)
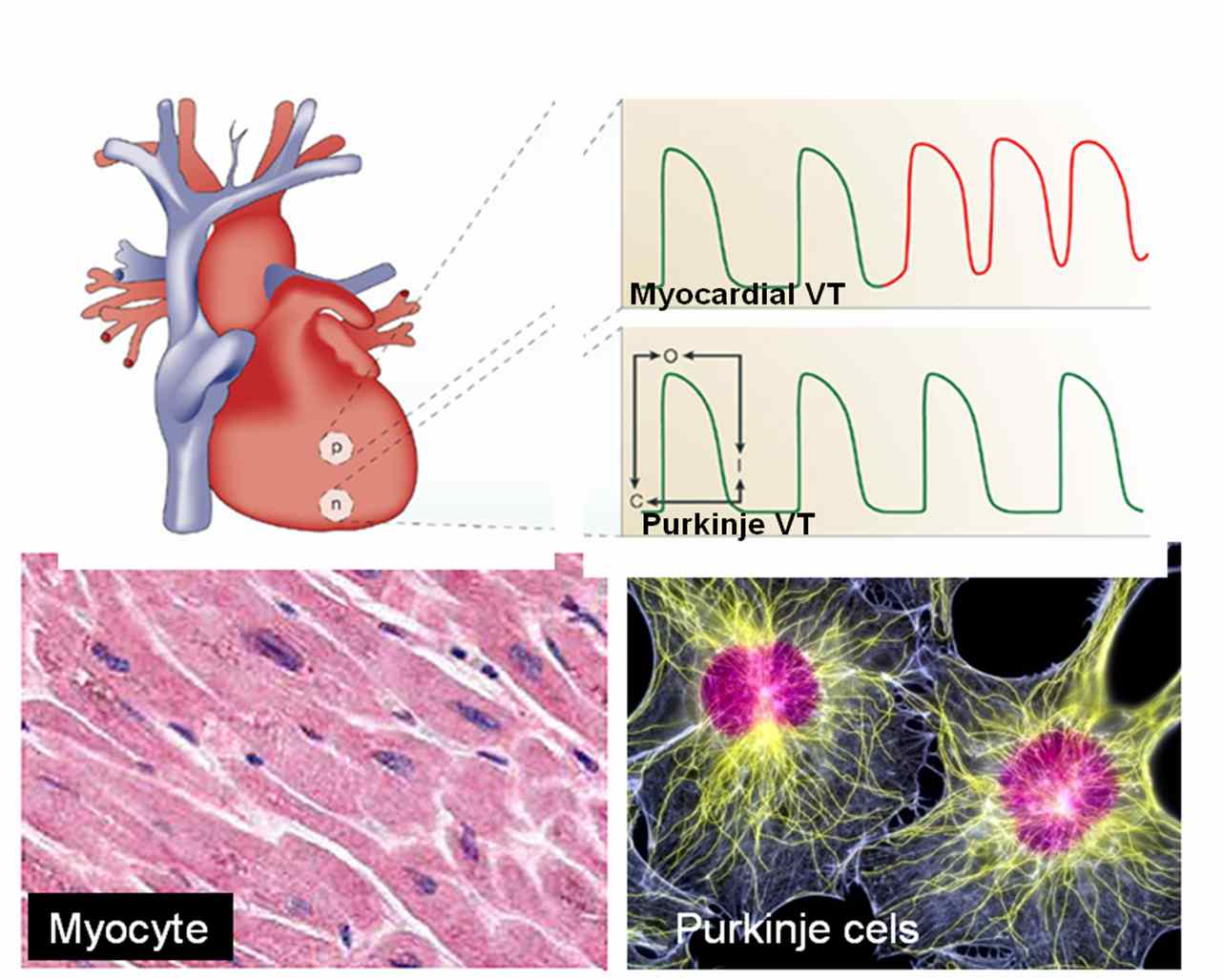
- Septal VTs*
- Fascicular VTs*
- VT in PPM and ICD /CRT patients **
* Any VT that arise near the major conducting system of ventricle conduct fast and hence qrs are relatively narrow.
**These are rare entities where base line wide QRS getting narrower with the onset of VT . (Ref : http://europace.oxfordjournals.org/cgi/content/full/eun254v1)
Wide qrs tachycardia >120ms
- Most of the genuine VT (Ischemic , myocardial origin)
- Post MI VTs
- SVT aberrancy especially AVRT
- Any SVT with preexisting BBB
- Marked electrolytic disorders
Unresolved questions
- Which lead we should look for measuring the width of qrs ?
- Should we take the narrowest qrs or widest qrs or should we take the average ?
- Should we calculate how much the tachycardia has widened the qrs from the baseline width of a given patient ? Is it not possible , what is wide for some may be normal for another !
- If there is no isoelectric line and ST segment blends with qrs complex how to mark end of qrs ?
- If limb leads show a narrow qrs and chest leads shows wide qrs what is the significance ?
- In precardial leads if one lead alone shows a narrow qrs , what is the significance ?
- Can a narrow qrs VT conduct with aberrancy and making it really wide ?
Final message
When we are able to solve complex electrophysiological problems , we must also realise even simple tasks can be demanding in medicne ! It is proposed to create a new group “Intermediate QRS tachycardia “that can help solve the issue where we have difficulty in labeling these tachycardias which fall in the greyzone .We can try & apply the modern EP based VT criterias to this group and find out the hidden truths !





{kind=link}