Murmurs are audible noises from within the Heart or vascular tree when blood flow loses its laminar flow and becomes turbulent. There are many factors responsible for it (Recall Reynold’s number ).It is obvious, that when there is hyperdynamic circulation, even in physiology one may hear a murmur. Pregnancy is a classical example and Innocent (still murmur) in children is another one.
Duroziez murmur: A brief history
In this post let us dwell on something about a classical murmur that occurs in the peripheral circulation away from the action-packed organ heart. It was originally described by French physician Dr Duroziez two centuries ago. (In his own words it was called a double crural murmur ). This happened shortly after Lennec’s new era of auscultation began. When everyone was concentrating on the heart Dr. Duroziez was curiously auscultating the legs and found this crural murmur. For this out-of-the-box thinking, he is still being remembered.
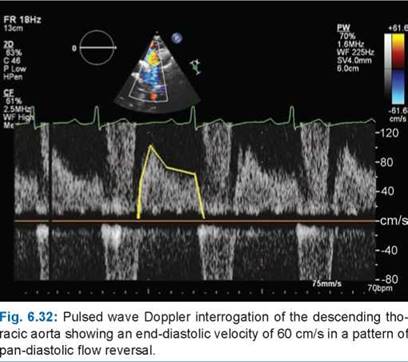
In significant aortic regurgitation, we know a substantial amount of blood regurgitates back into LV. This backflow though happens in the chest and into the LV, it is reflected all over the vascular tree. It so happens, the entire aortic forward flow for a moment slows in end-systole or even reverses at the end-systole and early diastole when the Aortic valve leaks. Almost all peripheral signs of AR are due to this. It is critical to remember, that these signs are heavily modified by arterial distensibility, associates obstruction, LV contractility, and peripheral vascular resistance.

Is there real reflux of blood back towards the heart* ?
Duroziez’s murmur remained controversial both for its mechanism and intriguing questions about, whether the blood really travels back in early diastole in the limbs or is just an acoustic illusion from a pressure wave. The debate was so intense it demanded a curious animal study. The femoral artery of Dogs with induced AR was injected with contrast and retrograde blood reflux was documented up to the iliac artery and Aorta.(NEJM 1965 Ref 1)
* While retrograde reflux of blood in the femoral artery is real, which manifests as EDM, we must understand antegrade diastolic flow murmurs or even continuous murmurs are common in hyperdynamic circulation over narrowed peripheral arteries and veins (venous hum)
**For Advanced readers: Some of the issues are not clear. Whether Duroziez murmur is truly decrescendo (Like its EDM counterpart in the Aortic area) or Is it mixed with antegrade diastolic flow murmur over the femoral artery due to hyperdynamic circulation.
Echocardiographic correlates of Duroziex murmur
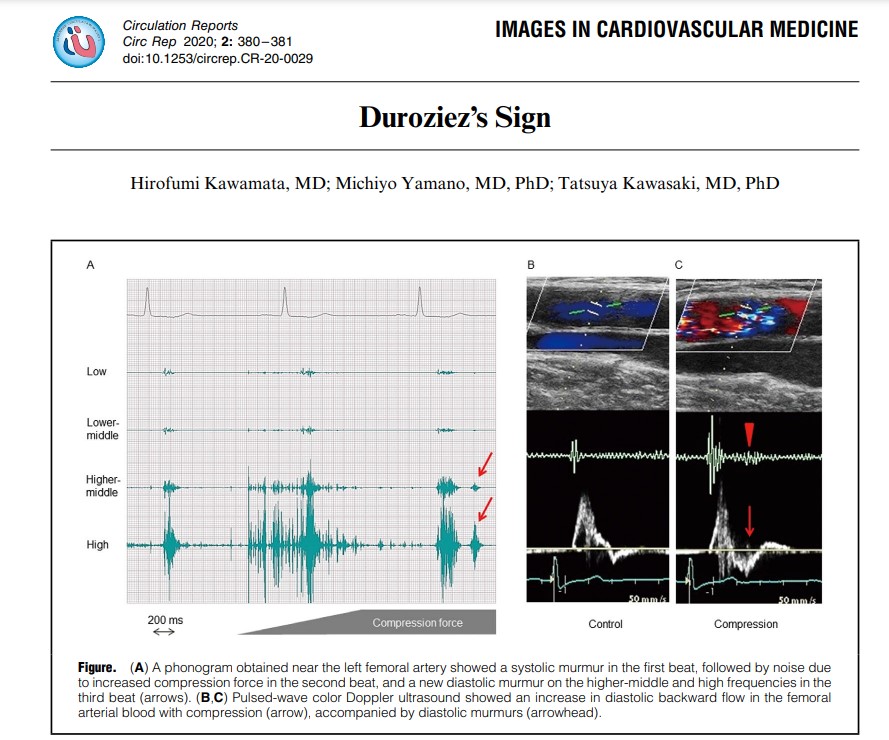
Now, we are able to document bizarre hemodynamics that happens the entire length of the vascular tree that is responsible for this murmur.(A related post 😦 In AR the run-off is central or periphery ?_)
Image courtesy: medmastery https://www.youtube.com/watch?v=eVhEXCO13ys
Phoncardiography with ECG correlation, help us to time the murmur exactly and also demonstrates reversal of flow in femoral artery by color flow doppler.
Importance of Duroziez’s murmur & A research proposal
Though it’s of historical interest, it is still discussed in exams. It may be amusing for the busy clinical cardiologist to auscultate over the legs, when they may be contemplating a TAVI for leaky Aortic valve (Arias EA, Interv Cardiol. 2019). But, for students, it is a different story. If anyone wants to beat the acumen and curiosity of Duroziez, they may assess the length of this murmur and correlate it with descending aortic flow reversal, aortic ERO, and regurgitant fraction. The fate of Duroziez’s murmur after Aortic valve replacement may also be studied.
Final message
Duroziex murmur is not just a vintage cardiac auscultatory sign meant for exam halls. Looking deep into it, we may get more insights into the behavior of the peripheral circulatory system in normal physiology as well as in patients with AR.
Reference
1.Duroziez PL. Du double souffle intermittent crural, comme signe de l’insuffisance aortique. Arch Gen Méd 1861; 17: 417–443,588–605.
2. N Engl J Med 1965; 272:1207-1210
3.Jama.1933.Blumgart and Ernstene