Not every one feels the palpitation during tachycardia / Bradycardia /VPDs , Why ?
Palpitation is awareness of one’s own heart beat. It is a complex perception of sensation at cortical level (like dyspnea) . It can occur during physical and mental exertion.However , if it occurs without any physiological reasons , it becomes abnormal. It can mean an abnormality in heart rate , rhythm or raise in stroke volume. The first rule of palpitation is both tachycardia and bradycardia can cause it. Tachycardic palpitation is due to valve motion and bradycardic palpitation is due to both motion and increased stroke volume.
The most common mechanism proposed for palpitation is hyperactive anterior mitral leaflet
How and where does the sensation of palpitation felt ?
Does it originate in the chest wall ? or Is it the vibrations spreading along the flow of blood in great vessels ? or Simply represent the vigorous valve motion sensed by Intra cardiac receptors ? How it is transmitted to spinal cord where it’s felt at cortical level ? We are not clear yet. Paccinian corpuscles is thought to sense these vibrations and hand over as electrical signals to spinal cord either directly from cardiac valves /walls or indirectly from chest wall.
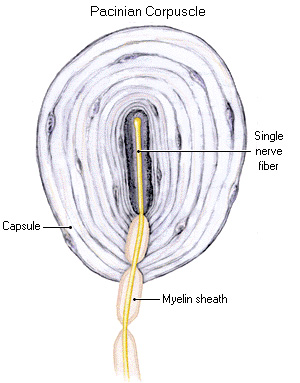
Paccinian corpuscles are predominantly present in sensory nerve fibres located in the dermis of skin. It is also observed in nerve ending to joints, Chestwall, blood vessel and also heart .They act like pressure as well as vibratory receptors * The exact reference for Paccinian corpuscle to be present within the heart is not available to me. Readers may contribute,
Importance of age and gender and IQ
Palpitation is primarily a symptom of young age where the heart is supple and more dynamic. Women tend to perceive more for some unknown reason. Elderly people rarely complaint about palpitation .It could imply aging with or with out autonomic dysfunction which suppresses transmission of palpitation signals to brain.Chest wall thickness also matters. My guess would be, Chest wall thickness, epicardial fat pad could absorb the vibratory energy and chest wall receptors fail to recognise it. One curious observation is, palpitation is described in a succinct manner by certain patients only. Since , it essentially involves higher cortical senses , we believe spatial intelligence of the patient may also be important.
Why Irregularity in heart beat is well recognized?
For the given heart rate , irregular rhythms are felt more often as palpitation than sinus tachycardia. This is the reason single ectopic beat is easily felt than sustained tachycardia. A common sequence of palpitation due to ectopic beat is , a suddenly missed beat, subsequent pause and forceful post ectopic beat.
Valve morphology and impact on palpitation
Mitral stenosis patients can feel their loud first heat sound (S 1) or varying S1 during atrial fibrillation as palpitation; Mitral valve prolapse with redundant , hyper kinetic motion is probably most common cause of benign palpitation.
Sclerosed and calcific valves attenuates palpitation. Calcific mitral valve in mitral stenosis make both S 1 intensity and opening snap feeble .These patients are less likely to feel palpitation .
Individual valve pathology can generate palpitation as in Ebstein anomaly , which has a the large sail like septal leaflet that flutters to create palpitation(Apart form pre-excitation syndrome common in this condition) As a general rule ,It is possible semi lunar valves are less likely to cause palpitation than AV valves as the latter only exposed to direct contractile pressure of ventricle.
Right vs left heart origin and localised palpitation
I am not sure one can differentiate left heart from right palpitation. But.palpitation arising from right ventricular volume overload and increased pulmonary flow like in ASD are associated with direct local sensation over pericardium . Mitral valve motion can not be localized by patients .However apical impulse can be felt.Neck pulsations invariably mean high flow states. Venous cannon waves due to high pressure tricuspid regurgitation can be felt with each heart beat (RV systole)
Exertional vs Non exertional palpitation
Palpitation occurring during exertion often imply its due to excessive handling stroke volume or (Pathological regurgitant volumes) Stenotic lesions are less likely to cause palpitation during exertion it’s never an absolute rule. Exercise Induced arrhythmia always happen in any valve lesions.
Relation with LV function
A dysfunctional ventricle cannot generate forceful contraction and hence palpitation is uncommon symptom. Cardiomyopathy presents with more of dyspnea rather than palpitation .Even, an episode of AF do not cause palpitation in such patients .They simply feel breathless (Dyspnea ? Or is it a palpitation equivalent ?)
New age palpitation
With so many foreign bodies and accessories entering the heart it’s not surprising for patients to feel amusing sounds and vibrations hitherto unknown in human body.
- Prosthetic valve clicks (Sounds from mechanical valves can be annoying .Tissue valves, TAVR are more quiet)
- Abnormal electrical activity from pacemakers and ICD coils.(Apart form pacemaker mediated muscle twitches)
- Now, we have entire mechanical LV assist devices working inside the heart with a 24/7 motors .(LVAD hum its called) Very soon heart is going to become a noisy place and patients would learn to ignore these abnormal sounds
Pleasant physiological palpitation
What brings the unpleasantness during palpitation? (applies to dyspnea as well). It is purely state of mind. While, palpitation due to extreme fear is unpleasant , palpitation due to pleasant emotional arousal (Often referred to as flying butterflies ! (Is it the wings of AML ? ) within the chest as we hear from some of young women & men ).Since they know the reason why they get it, cortical input welcomes it ,converts them to pleasant beats .The Non-academic stuff is intentionally made to understand how the limbic system and Hipocampus areas of brain can modify the incoming signals of palpitation that comes from down under.
Thoughts to ponder
Does post heart transplantation (De-nerved heart) patients experience palpitation ? Again, I am not sure .If palpitation is carried by cardiac nerves it should disappear. Of-course , 30 % of transplanted heart do get re-innervated. When you get a chance to meet a heart transplant patient you ask yourself and find the answer.
*Please be reminded Anginal pain almost vanishes post transplant.In fact ,there have been instances of cardiac auto-transplant for refractory angina in the past.
Final message
Though all of us can list causes of palpitation without any difficulty , we rarely dwell into exact the mechanism of genesis of this symptom and its perception. As we enjoy flying in an exotic world of cardiac interventions . . . the principles of practice of medicine also expect us to take adequate efforts to understand fully the cardinal symptoms of our patients . After all , they are the true teachers of Medicine. It is because of their pursuit for explanation for their symptom (Often vague though) we make our professional progress.
Further reading
John T.Shepard The Heart as a Sensory Organ JACC Vol. 5, No.6 June 1985:83B-878
(The heart has variety of sensory nerve endings , still to be explored)