Welcome to Kuna island. The Kuna Indians are really unique people. living off Panama, right in the isthmus connecting North and south America, The Kunas reside in the San Blas archipelago comprising about 360 islands, of which about 60 are populated by them. They have lived on these islands for centuries, but their exact origin is not completely understood.
These innocent tribes have taught an important lesson in human blood pressure regulation, vascular biology, and salt sensitivity. We know, that high blood pressure, is a maximally researched entity in medical science in terms of etiology, vascular effects, and its control. Still, we don’t know, what are the limits of normal BP for human beings. The debate will not end until we are clear about, whether human beings evolved from monkeys or emerged as de-nova organisms. Recent studies have revealed a remarkably low level of mitochondrial gene diversity in monkeys, suggesting that there has been remarkably little genetic admixture. (Ref 2)
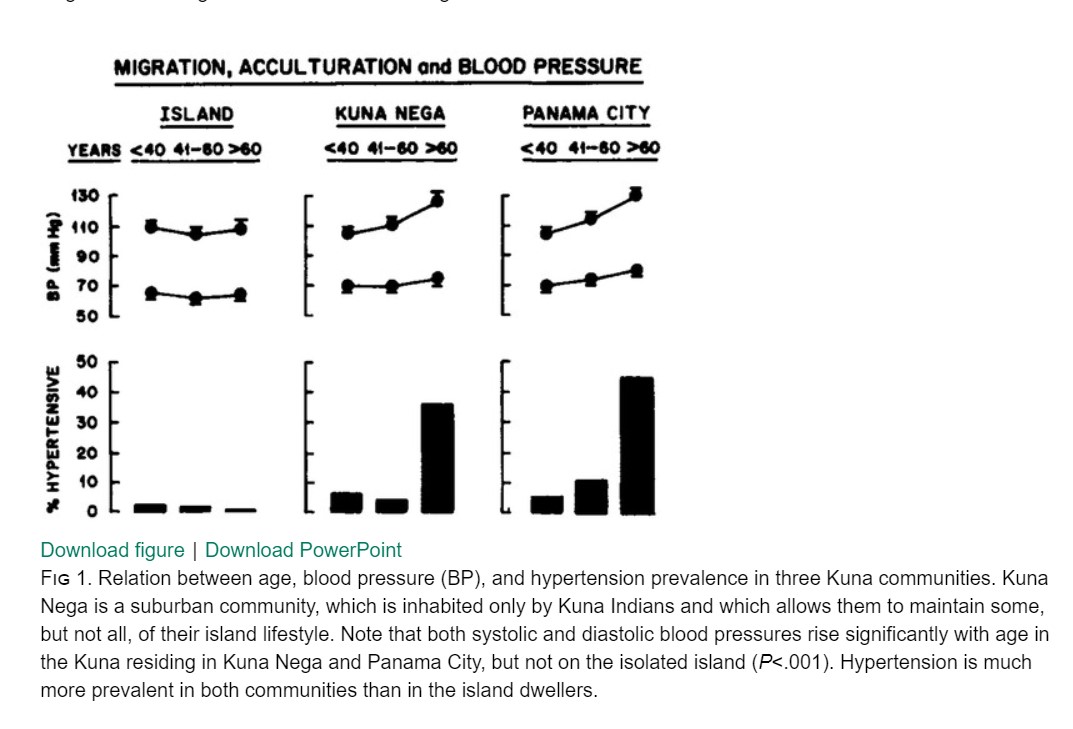
What we know from 3000-years-old human history is, blood pressure is directly related to the physical work done by us and the diet we eat. While salt is considered pro hypertension, physical activity is a much more important determinant in bringing it down. Normal BP in a pre-civilized world was low compared to a civilized population. They also enjoyed better vascular health. Where is the evidence? It comes from the life cycle of Kuna Indians. Here is a very unique paper published in the Hypertension journal.(Ref 1) Three cheers to the authors for confirming this long pending speculation with meticulous data collection. (See the Image)
What was special in Kuna’s diet that prevented cardiovascular events? It is been shown in the study by Hollenberg, their diet contained rich in cocoa and flavonoids that made the difference.(The salt consumption was still high though)
As Kuna’s moved out from their primitive lifestyle to first, the Kuna Nega,(a suburb) and subsequently to a fast-paced Panama city. See the impact on their systole and diastolic stress on the heart. The loss of protective effect of the native diet is obvious.
Final message
Lifestyle is the buzzword today. It is a by-product of the new civilized world that will define human health. The human vascular tree tries to sync with a new lifestyle pushing the BP curve to the north. The true normal BP for denova-human beings may still be very much lower than what we believe. A crazy suggestion was made, that human BP should match that of non-sedentary monkeys. I Hope, we get more evidence later for such hyperboles. As of now, we have to accept, hypertension is largely due to disorder in human civilization, development, and prosperity.
How about embracing the styleless lives of native Kunas to take control of our vascular health.
Reference
BROWN (S.), ATKINS (C.), BAGLEY (R.), CARR (A.), COWGILL, DAVIDSON (M.), EGNER (B.), ELLIOTT (J.), HENIK (R.), LABATO
(M.), LITTMAN (M.), POLZIN (D.), ROSS (L.), SNYDER (P.), STEPIEN (R.) – Guidelines for the Identification, Evaluation, and
Management of Systemic Hypertension in Dogs and Cats. J Vet Inern Med, 2007, 21: 542-558