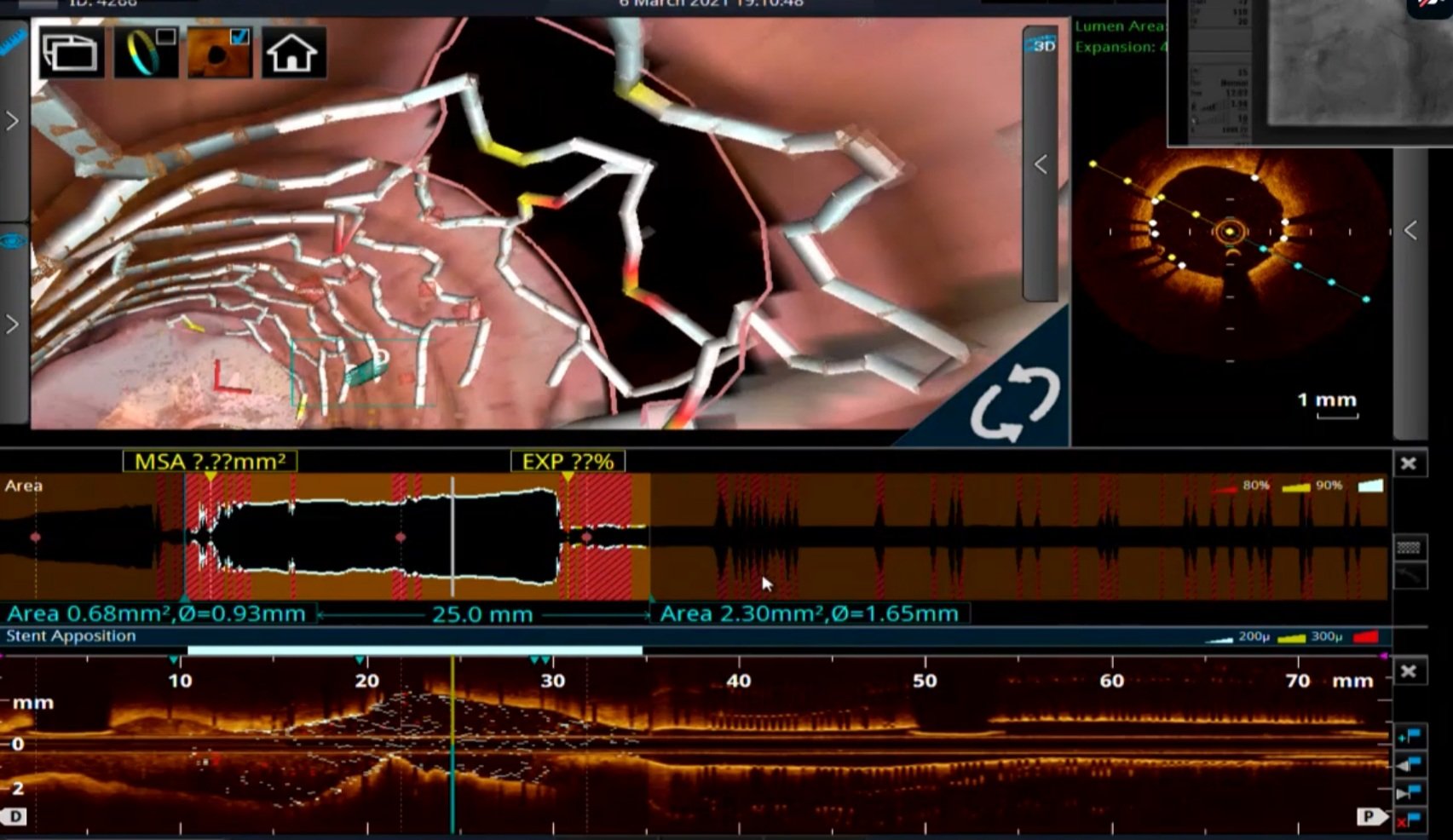
This is the story of PCI to LAD from the customary bifurcation workshop for the budding experts, which ended up with a compulsive final OCT run-through, triggering a debate on what to do with the side branch.
- Just balloon dilate the distal strut
- Would consider a second stent. Maybe a TAP depending upon LCX morphology
- At this stage, I would like to know the FFR or iFR across LCX Jail.
- Get rid of this OCT, Let me have look at regular CAG. I bet I can make a better decision.
- Leave it alone if the clinical status & profile is good
Leave it alone? Is it not an incomplete Job?
Definitely incomplete. Please realize, No job is complete in interventional cardiology. If we believe so, it exposes our Ignorance ( & some arrogance). Intentional side branch jailing is an integral part of PCI techniques. Are we not ignoring day in and day out.
Someone in the audience asked Why did you do OCT at all?
The chief operator quipped “You can’t ask this silly question in a scientific workshop. We bought the OCT kit to improve the quality of PCI. We are proud of it. Really feel blessed to use it and I am sure my patients will benefit from it”. We have to agree with him. These new Imaging techniques though give us extra high-definition, but it comes with troubling revelations with their new vision. If you are pathologically honest and believe in empowering patients, it is absolutely necessary to convey the following facts in the discharge record as well. It would be something like this, “There was a 120-micron strut crossing the LCX ostium, that might continuously impede a chunk of platelets & RBCs every beat, for the rest of your life and might enhance the risk for thrombosis. (Of course, DAPT will take care of it and ask the patient not to worry)”
OCT: One-minute review
OCT is Indeed a stunning Innovation. It can be useful in all 3 phases of PCI. 1. Assessment and preparation of lesion bed. 2. during stent deployment and optimization. ,3. Post-stenting follow up. The technology has grown so fast, now angiographic co-registration and longitudinal frame reconstruction comes inbuilt. It required 3 versions of LUMEN study and a 4 th one (LUMEN 4 ) is yet to come, expected in 2022 to prove the worthiness (or worthlessness) of OCT.
One attractively named DOCTORS study asked the specific question directly (Does Optical Coherence Tomography Optimize Results of Stenting)” This is from NSTEMI patients .read yourself for the conclusion. It is not convincing to me. DOCTORS study (Does Optical Coherence Tomography Optimize Results of Stenting)”. Circulation 2016; 134: 906.
Mind you, OCT is not only an expertise-dependent procedure, it also has important imaging limitations. It has low penetration max 2mm, can not differentiate lipids from calcium, shadowing behind red thrombus is an issue and most importantly it may miss the external elastic lamina (EEL) and measurement errors are real.
Cost-effectiveness
If an imaging technique to assess a stent *(*Still waiting to prove its worthiness) could cost more than the device itself, realize how good our economic intellect is. Just because your lab has an OCT console, it need not transform into a technically perfect PCI. There are at least half a dozen factors other than Imaging that matters.
Final message
OCT is a breakthrough technology that needs to be used judiciously and it definitely helps us understand the nuances of coronary stenting, especially in complex lesion subsets, and its mechanical and histological contents. However, let us not propagate a false message, that without OCT we can’t perform a perfect PCI. Give due respect to all those sharp-eyed interventional cardiologists with good techniques, who can do a better job, beating the HD vision of OCT, with their native blindness.
Reference
Post-amble
Can you guess how many PCIs are done with OCT guidance globally?
It is less than 5 %. In India, it must be, I guess it is < 2% So, we are living in a terrifying world of coronary interventions, where 98 % of PCI is happening blindly, sub-optimally, and unscientifically., Data from CLI-OPCI registry adds more panic: Centro per la Lotta Contro l’Infarto – Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) registry: It says device-oriented cardiovascular event (DOSE) is high with OCT detected sub-optimal PCI.
So, what are we going to tell our patients who will undergo PCI (undergone) without OCT guidance in the past, present, and future?
Simply ask them to forget this OCT stuff. Just reassure them. Nothing will happen.



