I was recently asked to suggest a topic for debate on STEMI in a major Indian cardiology conference. I wished , this is what we should be mulling over, with a set of virtual guest lectures and special invitees from heaven ! Plenary session : State of the Art STEMI care Time : 11.AM , Speaker : Dr Hippocrates Topic : Aren’t we erring on either side of the Noble profession ? Moderator: Dr. William Osler Chairperson : Dr .Harvey Cushings, Dr,Sir Thomas Lewis ,Dr Paul Wood , Excerpts : “While , vast number of our country-men’s culprit artery doesn’t even get that mandatory Aspirin on time . . . an urban rich man’s distal non-culprit artery is decorated with a fancy bio-vascular scaffold making that innocuous lesion vulnerable in the process as well ! Aren’t we erring on either side in the Noble profession ?
Archive for February, 2015
A crazy cardiology tweet and a wish !
Posted in bio ethics, tagged cardiology tweet, ethics in cardiology, stemi care on February 27, 2015| Leave a Comment »
Atrial fibrillation during STEMI : Don’t get alarmed
Posted in Atrial fibrillation, Infrequently asked questions in cardiology (iFAQs), tagged atrial fibrillation, atrial fibrillation in stemi, management of atrial fibrillation during stemi on February 25, 2015| Leave a Comment »
Atrial fibrillation is the most common arrhythmia we encounter in clinical cardiology .Ironically it is uncommon during ACS and extremely rare in association with UA/NSTEMI. Surprisingly , an entity ” Ischemic AF” is not to be found in cardiology literature.
The incidence of AF in STEMI is less than 5%. Occurs more often due to factors other than primary ischemia of atrial musculature. Of-course , AF in association with Infero posterio MI and RVMI is an important trigger for AF.LCX disease is more often associated with AF as it gives up a consistent branch to left atrium.
Though it is tempting to implicate ischemia as a trigger for AF ,most often it occurs , in elderly ,associated COPD ,hypoxia preexisting atrial disease .Acute elevation of LVEDP and stretch of left atrium could be a more logical mechanism.
Hemodynamic impact
- AF can bring down the blood pressure.
- Worsen ischemia by increasing the MVO2
- Could be very destabilising in RV infarction
- Surprisingly it is well tolerated in many STEMI patients.
AF in STEMI- Is it an emergency ?
It would appear so. But , if hemodyanmicaly stable one need not panic.Many times they are transient .Correcting hypoxia, optimizing beta blocker would help.
Role of DC Shock , Precautions before shocking & Post shock events
- DC shock is done only if there is hemodynamic instability or ongoing ischemia .(Very difficult to rule out the later )
- Mural LV clots can form even within 24 hours and DC shock embolic strokes may ensue .
- Hence it is mandatory to do an echocardiogram prior to shocking.
Drug of choice
- Betablocker
- Class 1c -Flecanide.
- Class 3 -Amiodarone./Ibutilide/
Role of Digoxin
There used to be a concern about usage of Digoxin in the setting of ACS as it pro-arrhythmic , but it remains useful in the management of AF .There is no other anti-arrhymic drug available to control, the heart rate without depression of the LV function
Rate control vs rhythm control
Always aim for rhythm control in the setting of ACS.Rate control is may not be a logical concept in acute settings though Amiodarone does both.
Wide QRS Atrial fibrillation
As we know , AF in STEMI can conduct with aberrancy , and we have a traditional teaching all wide qrs tachycardia are VT in the setting of MI making our patients statistically vulnerable.
After all , both entities lack discernible p waves. At high rates it may be difficult to identify irregularity RR interval. However , one would shock such patients and both AF and VT would respond .All is well that ends well.
Summary
AF during STEMI is a risky arrhythmia and needs urgent intervention , but one need not be alarmed .There is a set of protocol . Only hemodynamically unstable AF require DC shock .Many times it is just transient.There has been instances of physician panicky that has resulted in more adverse events .
Forward looking IVUS : A catheter with a camera on its leading edge !
Posted in cath lab tips and tricks, ivus, Newer technology, tagged cmoc ivus catheter, cto intervention, forward looking ivus catheter, ivus, tips and tricks i ivus on February 22, 2015| 2 Comments »
Cardiologists do magic inside the human coronary artery , that too in a live beating heart , unlike the surgeons.Blocks are removed , holes are closed, valves are inserted , scars are burnt, new electrical connections are laid .They do this with relative blind vision with good degree of success. Still, as we aim for more precise interventions we require excellent imaging modalities to assist us.
In PCI of CTO(Chronic total occlusion) the critical element to know is the morphology of the tissue plane , what exactly we burrow ? as we navigate through complex, often hard shapeless tortuous tissue tunnels . Our patients will be surprised to know we are currently doing this with our eyes shut. If only we have a camera guide in the tip of the wire it give us tremendous advantage .
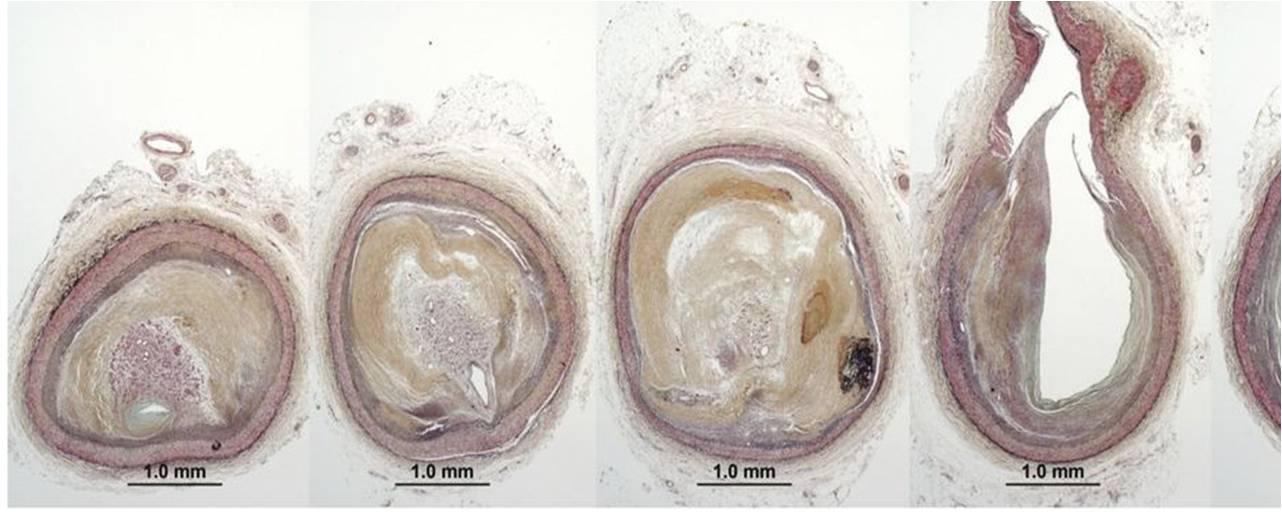
The CTO morphology .Image source : Kenichi Sakakura ,Eur Heart J. 2014 Jul 1;35(25):1683-93.
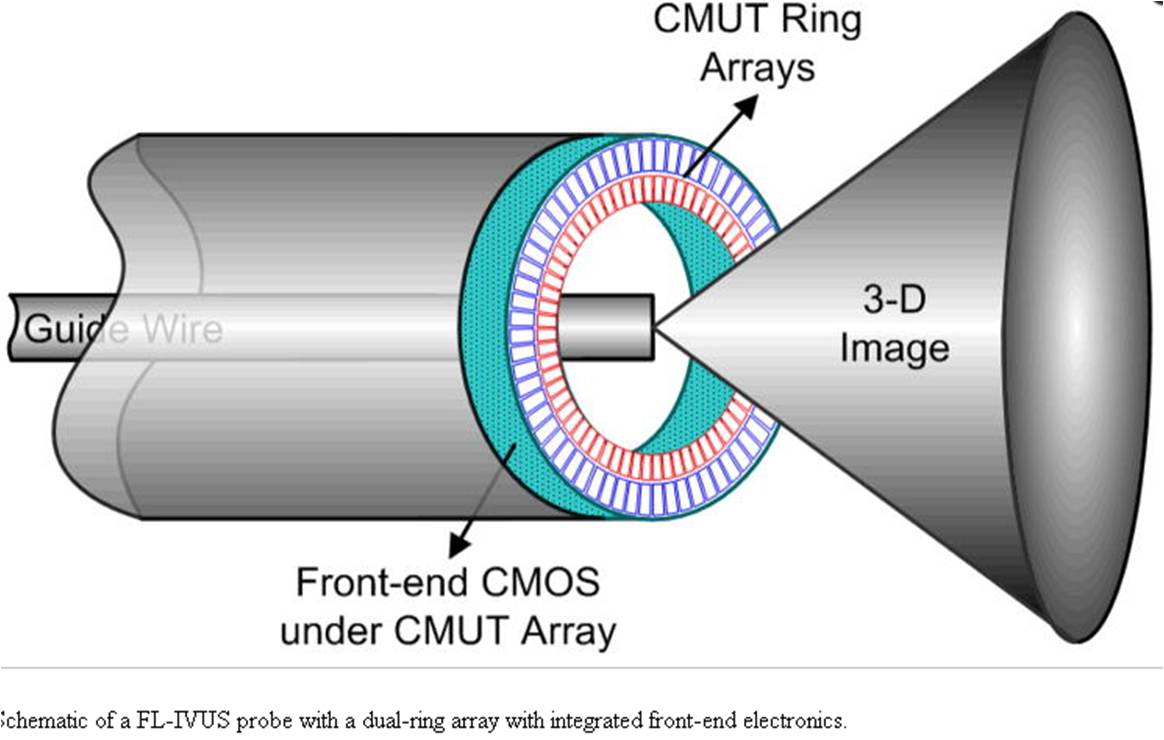
The exiting IVUS technology can only look sideways . Now a new vision is added by annular array of transducer at tip with CMOS sensor .The technology is just coming out it would be use for us in the near future .
Anatomy of the forward looking ultrasonic eye
Reference
I am confused sir , what is the hierarchy of medical advisories ?
Posted in Cardiology -guidelines, Infrequently asked questions in cardiology (iFAQs), tagged evidence based medicine, guidelines vs recommendatios, instituional protocols, medical ethics, protocols on February 21, 2015| Leave a Comment »
In this era of synthesized evidence base, one of my intellectually aberrant student asked How can we indulge in a popular coronary procedure with class 1 indication backed by level C evidence ? (As defined by the seemingly invincible guideline committee of various International cardiology organizations .)

I told him ,
- Institutional protocols are to be followed
- Guidelines are to be respected
- Recommendations are to be considered
- Please be reminded all of the above can be rejected outright !
Finally , realise Individual decisions based on sound scientific understanding with zero non academic intrusions will be revered forever !
*Caution : If you think you haven’t yet reached that the level of individuality , come what may , you are expected follow these advisories which are primarily aimed at providing quality care and you will be pardoned of any adversaries as well !
Pulse rate in ventricular bi-geminy : A missing link ?
Posted in Auscultation, Cardiology -unresolved questions, tagged absent s 2 in pulse deficit, effect of vvpd on aortic and mitral valve closure, heart rate in bigeminy, mechanism of pulse deficit, more s1 and less s2, paired pacing and vpds, pulse deficitin bigeminy, pulse rate in bigeminy, ventricular bi-geminy, ventricular ectopic beats on February 17, 2015| Leave a Comment »
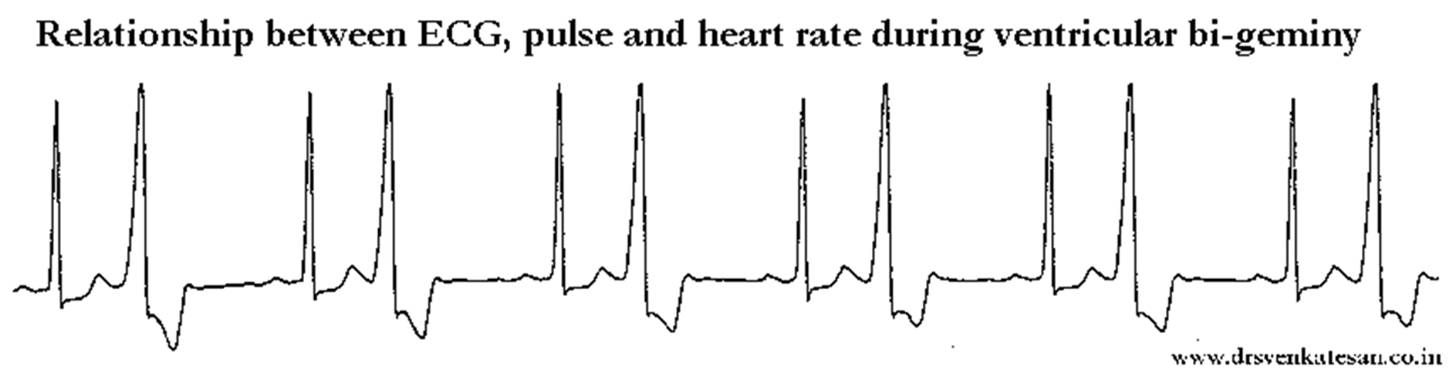
Answer : Most probably B .
What we feel in peripheral pulse , is one weak and the one strong beat in sequence .The later is due to post VPD potentiation. Since there is a compensatory pause , ECG rate (Number of QRS complexes /mt) and pulse rate are same .
Ironically , heart rate and ECG rate are not same as VPDs impact mitral valve more than aortic valve and cause additional S 1 than S 2 making heart rate considerably more than pulse rate and logically it must be double the pulse rate . This may be difficult to appreciate by auscultation, but can be documented by phono-cardiogram or by M mode echocardiogram.
Determinants of gradient across coarctation of Aorta
Posted in Aortic diseases, coarctation of aorta, Infrequently asked questions in cardiology (iFAQs), tagged coarctation of aorta, collaterals in coarctation, cp stent in coarctation, effect of bicuspid valve on coarctation gradient, effect of ht on gradient in coarctation, gradient across coarctation of aorta, mechansim of hypertension in coarctation, renal hypertension in coarctation on February 16, 2015| Leave a Comment »
The gradient across coarctation is not simply (& solely ) determined by degree of obstruction , as one would believe.Understanding the hemodynamics and various factors that can influence the gradient is essential Relieving the obstruction /gradient by stent or surgery may not be synonymous with successful treatment as we understand now the entire aorta right from the root to abdomen can influence the gradient ,along with systemic factors.We also know , some of these patients harbor histological abnormalities in the entire stretch of Aorta , what is being referred to as pan aortopathy , that may influence the long-term outcome.

It looks like adult cardiologist should avoid doing pediatric echocardiograms !
Posted in bio ethics, Cardiology -Therapeutic dilemma, cardiology-ethics, tagged adult vs pediatric echo report, echocardiography expertise required, errors in echo report, errors in echocardiography, ethical issues in cardiology, inadequate echocardiogram, incomplete echocardiogram, mistakes in echo report, pediatric echocardiography who should do ? on February 14, 2015| Leave a Comment »
A cardiologist is a physician who has trained himself in a special way to deal with any problem of heart.Ironically , it exists only on paper.The field has developed so vast no one can master everything .There is no such “Pan or global cardiology expert” .In fact it would be shortly become unethical to try to become one !
Pediatric cardiology has developed into such a big field , doing a echo in newborn or infant has become a comprehensive job and requires special talent .This unique and excellent study from Narayana Institute , Bangalore published in the prestigious Annals of pediatric cardiology throws up interesting realities about the quality of echo report done by adult cardiologists in children .The error rate appears huge and stands at prohibitive 38%. While many errors were minor , major were also not insignificant (23%)

With bulk of the pediatric echo involves in the critical decision making process of device closures and interventions the data required becomes vital .The commonest cause for error is probably not due lack of knowledge and but to due to lack of commitment and continuous exposure in doing echocardiograms in those age group.
While this paper decently skirts the issue of quality of pediatric echo done in medium sized hospitals without pediatric cardiology service ,I can say the error rates or inadequate reportage could be significant in such hospitals with apparently good ranking .
Final.message
Of course ,we have many adult cardiologist who do excellent pediatric work , It looks like , as a general rule performing pediatric echocardiograms by non -institutionalized adult cardiologist may not be appropriate ! It may be wise for them to avoid doing echocardiogram in small infants with truly complex disorders (even perceived complex) till they gain the required expertise and confidence.
I recall an adverse issue happened years ago , when I had missed an associated PAPVC in ASD that made my surgeon anxious on table .In a country like ours there is no one to audit our work , “our conscience remains the only option” to deliver the best for our patients especially so, when they are tiny lives in distress.
After thought
Who am I to suggest who should do echocardiogram ? , after all every cardiologist is licensed to do that . One simple suggestion would be , if not confident they can at least mention in their report it is only preliminary evaluation and need to be followed up with an expert . I do that whenever its required and gives me peace of mind as well !
More controversies* to come
Can adult cardiologist do pediatric intervention ?
* Controversy : One of the meaning for this word is “It is a thought process set into motion , that aids digging up hidden truths ”
Reference
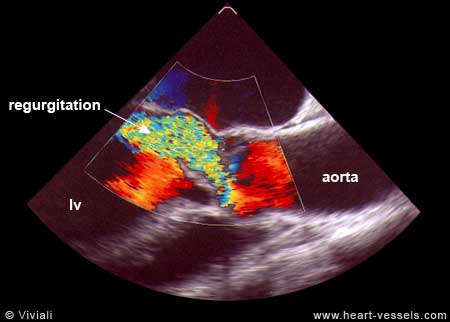
Where is the run off in Aortic regurgitation ? Is it central or peripheral ?
Posted in Aortic diseases, Aortic regurgitation, Cardiology - Clinical, tagged arterial pulse in aortic regurgitation, diastolic run off in aortic regurgitation, mechanism of collapsing pulse in aortic regurgitation, peripheral run off, peripheral systemic arteriolar dilatation in aortic regurgitation on February 13, 2015| Leave a Comment »
We know aortic regurgitation causes a deluge of hugely popular peripheral signs of aortic run off , which are taught right from 2nd year medical school.
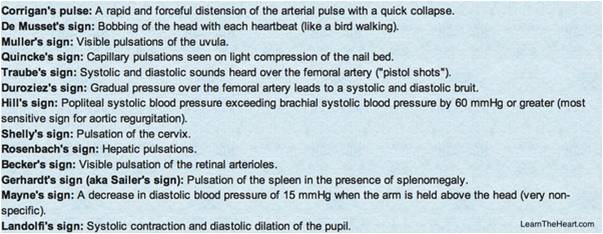
When the aorta leaks it reflects in the entire vascular tree .How is that a leak in the remote aortic valve cause a quincke’s to and fro pulsations in the finger pulp ?
Is the blood in the finger trying to follow the regurgitant jet that go back into left ventricle ? Does the to and fro murmur of Duroziez over the femoral artery imply there is reversal of blood flow in femoral artery ?
Things are little complex than it appears
It is true the initiating event of collapsing pulse is the regurgitant jet , however the mechanism that amplifies and sustains it , lies in the altered peripheral hemodynamics.
The systemic arteriolar resistance is dramatically low in chronic severe AR by a reflex phenomenon , as cardiac out put is increased and vascular tree adopt to it. So, with each beat when blood is ejected two things happen in diastole .While a small fraction runs back into LV , the rest of blood runs off , as if it goes in a free way making all peripheral pulses dynamic , bounding and collapsible.
Hence as the name suggest all the peripheral signs of AR are due to the peripheral mechanisms rather than primary event of aortic run off into left ventricle.
Why carotid pulse does not show the collapsible nature of pulse in AR ?
If aortic leak into LV is the dominant mechanism , carotid artery should obviously manifest a collapse ,but it doesn’t ,as carotid has no direct continuity with the peripheral low resistance circuit
What is the hemo-dynamic correlates of descending aortic flow reversal in severe AR ?
The central vascular tree manifest some reversal till the regurgitant velocity fades off . This can occur in severe AR, extending into certain length of aorta. This can be picked up by Doppler probe. Please realise it is only the wave form that get reversed not the actual blood stream.( The momentum gained in systole continues to push forward in-spite of the pulling back forces of regurgitation)
Why peripheral signs are absent in acute AR ?
Acute AR even if it’s significant does not cause a collapsing pulse because it takes time for the peripheral vascular tree to go for vasodilatory mode.Further ,LV is also less compliant keeping the LVEDP high and regurgitant fraction low.
Summary
Answering the title question ,the mechanism of Aortic run off in AR is both central and peripheral. However clinical signs are largely due to high cardiac out put and the resultant adaptive response of the vascular tree due to low systemic vascular resistance triggered by reflex dilatation of small arterioles of the peripheral vascular bed.
Ignorance based Electro-physiology : Why chronic RBBB is a benign entity ?
Posted in Cardiology - Electrophysiology -Pacemaker, RBBB/LBBB, tagged bundle branch reentry, eelctrophysiology, electrophysiology, ers pattern, moes theory, rentry mechanism, sloe conduction and reentry, theories on genesis of cardiac arrhythmias on February 12, 2015| Leave a Comment »
In the last few decades we have understood a major concept in the genesis of cardiac arrhythmia.Slowing in the propagation of cardiac impulse is a key trigger to precipitate a reentry circuit and initiate a tachy- arrhythmia.Still , many conditions like first degree AV block, chronic RBBB or even LBBB are benign entities as along as the heart is structurally normal .They seem never increase the incidence or life time risk of cardiac arrhythmia . Longevity is unaffected.( Or do we assume many things ?)
How is this possible ? or is the theory of slow conduction triggering reentry is flawed ?
Think again . . . if these patients who later on develop a structural heart disease , with an episode of ACS , myocardial or valvular disease, the original slow conduction substrates these people were harboring , will it become important ?
Surprisingly , we have no answers in literature.When Haissaguerre et al found preexisting ERS pattern could be a trigger for primary VF in case they develop ACS , he opened up a huge debate as it involved converting a vast number of normal population electrically anxious.
Now ,is it possible the so called benign blocks of heart like first degree AV blocks , RBBB , LAHBa , would be important at times of ACS and possibly make them prone for for primary ischemic arrhythmia .
Is bundle branch re-entry possible in structurally normal heart ?
We need answers. Some one , (Any EP fellow) somewhere could take up the issue and enlighten us !
Innovation in pacemaker battery technology : ICDs go slim and live longer !
Posted in Cardiology - Electrophysiology -Pacemaker, ICD -Tips and Tricks, ICD and Pacemakers, tagged aicd mirowski, boston scientific icd extedended life, el icd dynogen inogen, icd indication, life of icd, madit study icd on February 10, 2015| Leave a Comment »
ICDs are one of revolutionary devices , invented last century that can defy “death & fate” in high risk cardiac patients who are threatened with ventricular tachycardia or fibrillation .A decade long hard work by Mirowski and team from John Hopkins culminated in the dramatic the first AICD implant in 198o. ( In my opinion, this medical invention can be compared to an event of such significance as moon landing by Armstrong and team ! ) Ironically , in the last decade such a revolutionary device was sort of misused and thousands of devices were explanted for inappropriate indications.
Fortunately , better sense prevailed recently .The indications are getting refined. I am sure ICD will go a long way in prevention of both expected and unexpected sudden electrical deaths .We are into the 4th decade of its evolution.While the electrical circuitry has been mastered , power supply remains an issue as they require continuous power supply like a mobile phone. Current technology allows about 6-8 years of battery life.

Now , Boston scientific has come out with new technology which make its battery life extend by 100% to 12 years. It is a major break through , expected to evolve further until probably we have rechargeable batteries or biological power sources .Stretching a wild thought , the days couldn’t be far off when the smart phones which are omnipresent in every human-being , could not only power the ICD remotely and control it too !
Indications (ESC/AHA 2012)
CAD
- Post MI* /LV dysfunction ≤ 35% /NYHA class II or III (* > 40 days)
- Post MI* /LV dysfunction ≤ 30% /NYHA Class I (* > 40 days )
- With non-sustained VT due to prior MI, LVEF < 40%, and inducible VF or sustained VT at EP study
Non ischemic structural disease ( Idiopathic DCM, ARVD etc)
- With structural heart disease and spontaneous sustained VT, whether hemodynamically stable or unstable.
Primary electrical disease
- With syncope of undetermined origin with clinically relevant, hemodynamically significant sustained VT or VF induced at electrophysiological study
Reference
Link to Product manual form Boston scientific.
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- August 2026 (2)
- July 2026 (6)
- June 2026 (9)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,716,961 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

