Hypertrophic cardiomyopathy (HCM) is the most common primary cardiac muscle disorder.It is one of the extensively studied medical entity in terms of pathology, genetics, electrophysiology and treatment.Though it has dramatic myocardial phenotypic expression , longevity can be near normal except in a minority who are prone for LV dysfunction and SCD due to the indirect electrical instability.These arrhythmia arise due to myocardial disarray , micro vascular disease or fibrosis.
NSVT by definition is runs of VT at a rate of > 100 /mt occurring less than 30 seconds.
How common is NSVT in HCM ?
On Holter study with 178 patients with HOCM (Adabag JACC 2005 ) 90 % showed VPDs
- 12% > 500 VPDs/24 h
- 40% had couplets,
- 30% had non-sustained ventricular tachycardia (NSVT).
- Over a follow-up of 5.5 6% patients died suddenly (annual mortality rate, 1.1%)
For sudden death, NSVT on Holter ECG had negative and positive predictive values of 95% and 9%, and sensitivity and specificity of 45% and 69%, respectively.

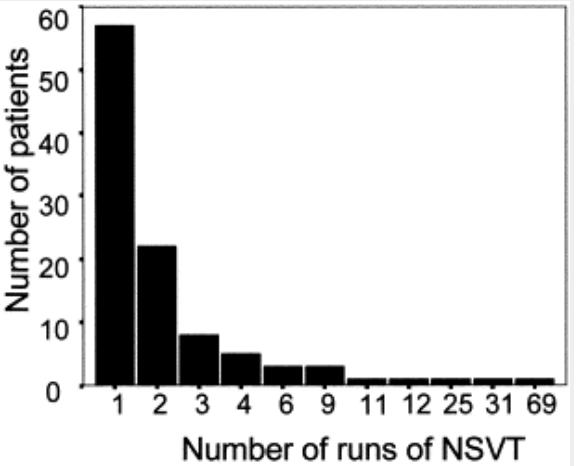
In this series from StGeorge hospital London from 630 patient incidence of NSVT was 19% and 4 episodes were observed in 48 hr in most .Monserrat L, JACC 2003
What is the duration , How fast and how frequent is the NSVT ?
It is expected the total burden of NSVT would have a definite impact on outcome. Curiously the duration, fastness and frequency of NSVT was not related to prognosis in atleast one study (Monserrat L, JACC 2003)
Relationship between age and burden of NSVT ?
Aging has a sobering effect on these ventricular ectopic activity by probable conditioning and fibrotic interruption of electrical activity.
How often a episode of NSVT convert to VT ?
Considering the day to day even it should be termed extremely rare . Even among person who survived an SCD the next episode of VT can be very rare.
What is the current Indication for ICD in HOCM ?
Secondary prevention (Consensus > Controversy )
Primary prevention (Controversy > Consensus – Still evolving )
Questions galore . . . answers struggle !
Does NSVT arising from single focus or multiple focus ?
What is the relationship between NSVT and degree of obstruction ?
What is the relationship between NSVT and MRI detected myocardial scars ?
How effective is beta blocker suppress NSVT ?
Can we implant ICD for only NSVT ?
Is it true ICDs add more anxiety , distress and harm than the index disease ?
How to program ICD to ignore NSVT and fire only for VT ?
For further information , refer this most authentic knowledge base. 
Final message
Predicting which NSVT will go for SCD in HOCM can be as difficult as predicting the next major earth quake that would strike the pacific rim that experiences unrecognized tremors on everyday basis .We have learned to live with that right ? So it appears NSVT is more of a nuisance arrhythmia for both the patient and physician .
Still , science demands identification individuals with highest risk for arrhythmia . How to do it ? Is it the morphological features , degree of obstruction or genetic finger prints. It is still not resolved . One thing is clear we can’t advice ICD for all those with runs of NSVT for perceived fear or pressure from peers or industry !
Referene
6. O’Mahony C, Lambiase PD, Rahman SM, et al. The relation of ventricular arrhythmia electrophysiological characteristics to cardiac phenotype and circadian patterns in hypertrophic cardiomyopathy. Europace 2012;14:724–33.
Read Full Post »