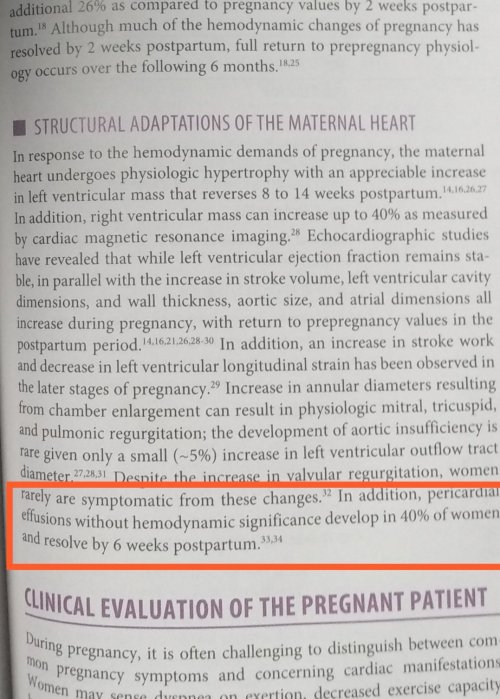
Pericardial effusion can be detected in many normal pregnancies. The Incidence is up to 40%.The normal fluid within the pericardial sac is around 25ml. A thin sheet of echocardiographic fluid collection in diastole up to 5mm is considered mild.
A trace or minimal effusion may be a better terminology that describes most physiological pericardial fluid compartment. They have no physiological significance.Mechanism is due to overall increase in size of vascular compartment and especially the right heart volume overload.
Pericardial fluid drains through systemic pericardial veins and lymphatic channels also drain into venous system through thoracic duct . In pregancy these drainage pumps work overtime at its peak capacity. It’s natural it might get fatigued and show some residual fluid collection which should never exceed mild.
We also know thyroid hormones is one of the housekeeping hormones within the pericardial space.Physiological hypothyroid state is possible.Effusion in true pathological Hypothyroidism causes secondary dyslipidemia. Here, some unknown lipid sub-particles clog the lymphatic and cause pericardial effusion which is actually a part of widespread systemic edema. (Myxedema)
https://www.ncbi.nlm.nih.gov/m/pubmed/12756478/
Reference Hurst’s The Heart Valentine Fuster Mcgraw Hill, 14th edition Page 2347
Read Full Post »