News: Series of clinical trials fail to clear the ongoing confusion in the business of cardiac revascularization.FAME 3 is the new addition.
Caution: A non-academic journal review
There is no secret, about this cold war happening in an incognito mode for territorial rights between cardiologists and cardiac surgeons in glamorous cardiac suits for the past two decades. Of course, we keep believing this is a friendly fight in the overall interest of CAD patients. The ultimate winner should be the patient, not anyone else. Will that happen? Will anyone will allow that to happen? I am not sure.
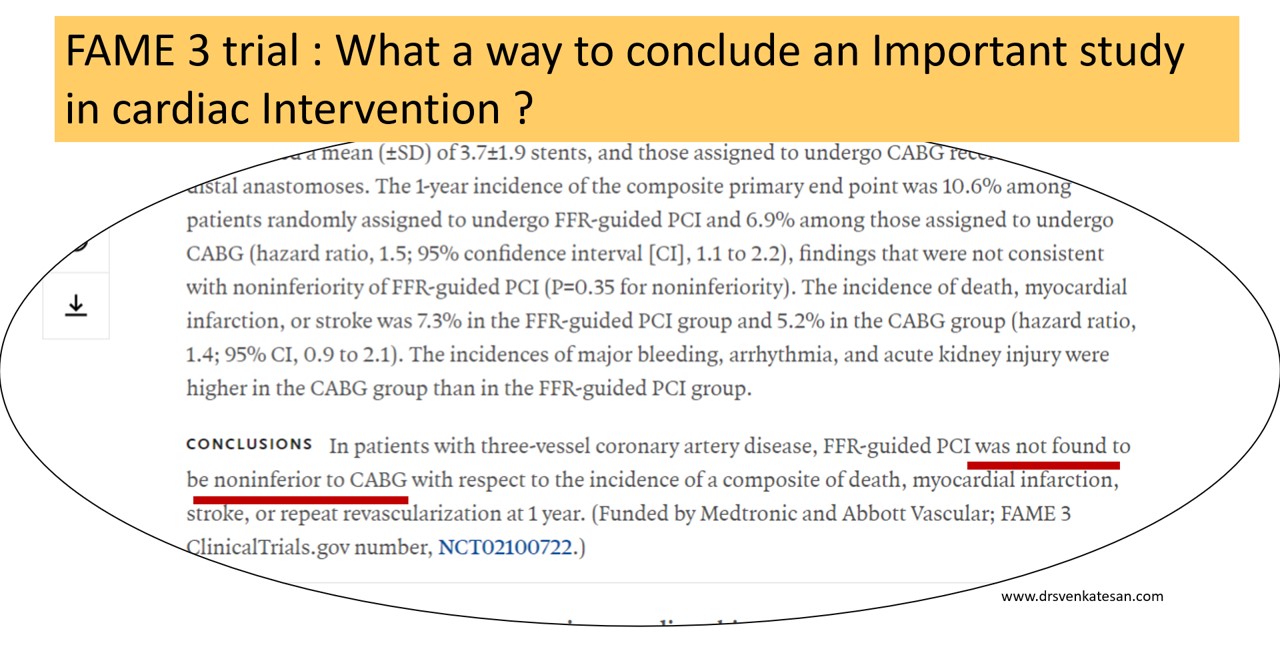
The FAME3 is a stunning large study from 50 centers FFR guided multivessel PCI, that failed to dethrone CABG (or at least it wanted to sit along with it) I am not a seasoned statistician but definitely can’t understand the logic behind the methodology* and the choice of words in the conclusion from a paper published from a renowned journal.

(*I can recall an article about Non-inferiority trial from Lancet (Ref 1) )
FAME 3 aftermaths: A dizzy Interpretation
Before accepting the fact that, FFR guided PCI wasn’t able to show its superiority or to unable to prove its non-Inferiority, while CABG was clearly found to be non-inferior, (rather superior) to PCI, we should take into account an important caveat in the concept of FFR itself, which has at least half a dozen serious hyperemic and non-hyperemic flaws that demanded a more superior,non-hyperemic indices like iFR, RFR, qFR, etc.
Those of you who still believe PCI would be an undisputed modality in multivessel CAD should take up the challenge and disprove the superiority of CABG by doing the same FAME 3 subset with iFR and other stuff. (Eagerly waiting for the hypothetical iFAME 4 trial)
One more way to Interpret FAME 3: How can we accept FFR guided multivessel PCI as inferior, unless we have an FFR guided CABG (FAME 3 didn’t do this) to compare? Can you guess if only pre-CABG FFR was mandatory criteria, that would have excluded or included important grafts, what would have been the impact of CABG? This is a more dramatic suggestion, that will say sorry to FFR,( the old physiological friend,) and label it as a new villain.
Final message
Multivessel PCI still has a long way to go before trying to dethrone CABG. But, strictly scientific cardiologists need not worry much and they can continue to indulge multivessel PCI without FFR, which is no longer unscientific ! Thanks to FAME 3. I think one of the Important indirect consequences (?purpose) of FAME 3 would be, playing the end game for FFR.
Reference

https://doi.org/10.1016/S0140-6736(07)61604-3
Read Full Post »