A 45 year old man came with recent onset breathlessness.His left ventricle was dilated along with left atrial enlargement.The LV EF was 42% (By current definition mid range preserved systolic function( Circ Heart Fail. 2016 Apr;9(4))
But, he was severely symptomatic because of combined systolic and diastolic dysfunction.Diagnosing and grading diastolic dysfunction has been extensively done in last decade.Now , we realise without significant diastolic dysfunction symptoms of pulmonary congestion can never occur in patients with DCM.
We don’t require complex tissue Doppler parameters to diagnose high-grade LV diastolic function.Just have a look at LA dimension, concentrate the E to A ratio. A tall E that humbles the A by more than 2 to 3 times is clear evidence for LA mean Pressure exceed 18 to 20 mmhg or so.
This , in combination with dilated LA is a marker of chronic severe diastolic dysfunction.The fact that A is diminutive in no way takes the Importance of Atrial contribution to LV filing at this critically compromised LV status.
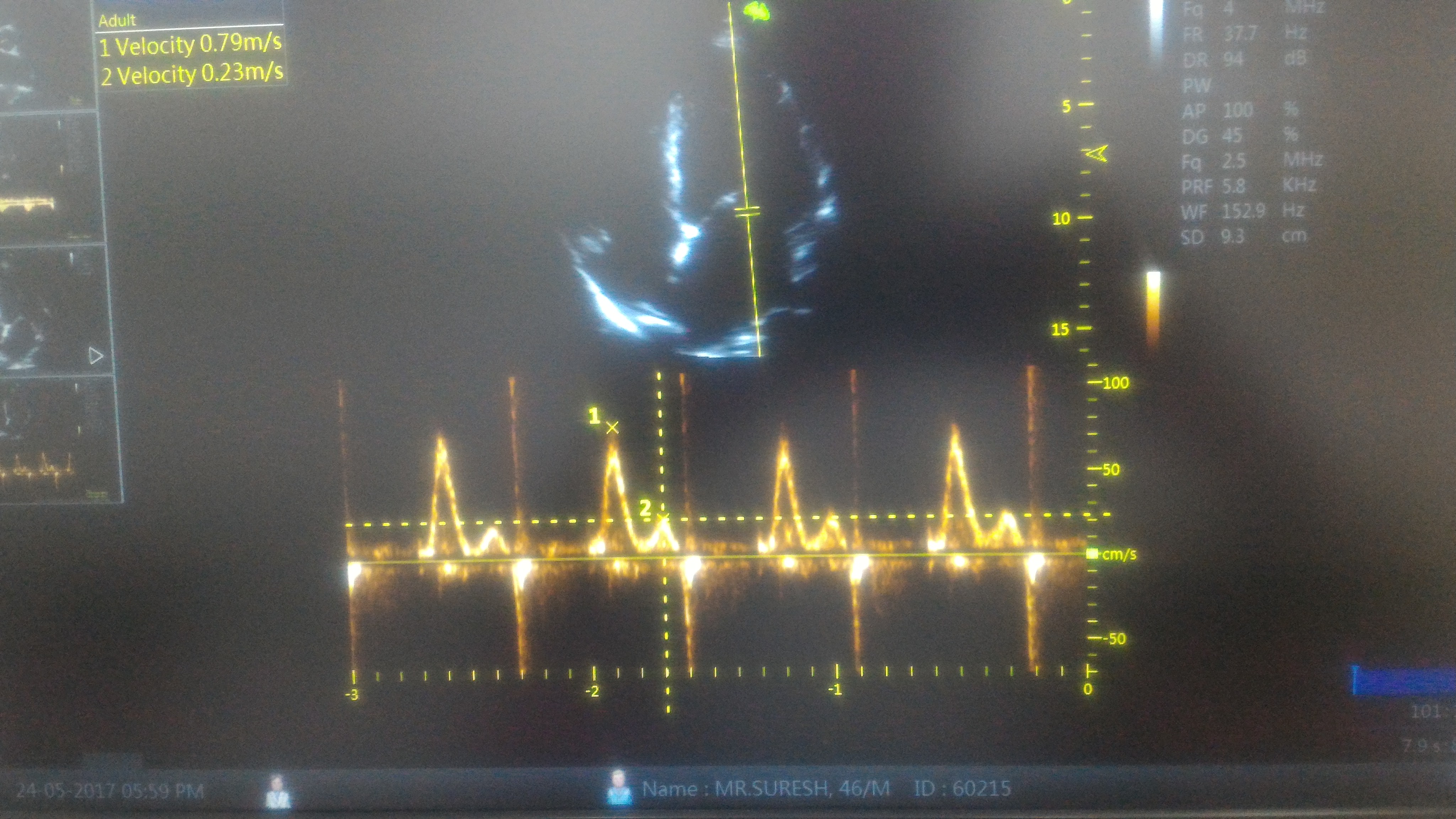
Note E:A ratio is 3:1 .This simply means the early (and mid to a certain extent ) diastolic pressure in LA is high and most of the filling takes place before Atrial contraction .There is one more reason for diminutive A . Atrial contractility fails to prevail over E in late diastole as LV end diastolic pressure is significantly high in these patients with diastolic dysfunction.

A dilated left atrium is an Independent marker of significant LV diastolic dysfunction (In the absence of MR) .When does LA begin to enlarge in diastolic dysfunction ? There is uniform rule.Generally LA size more than 4.5cm indicate grade 3 or 4 LV diastolic dysfunction.
LA size and Pulmonary congestion
It’s a paradox , a roomy LA dampens the LA pressure curve and A reversal into lungs may not happen.
*AF irony on A reversal
Logic might suggest , loss of atrial contraction might attenuate A reversal and less blood flooding into pulmonary veins.No, It doesn’t happen that way.If AF is precipitated for any reason its going to be “switch on” for acute pulmonary edema.
What is the relation between systolic and diastolic dysfunction in DCM ?
We find about 30 % of DCM has documented resting diastolic dysfunction.This is actually a underestimation of true diastolic dysfunction as it can very well manifest only during exertion.
Though generally , there is good correlation of grade of diastolic and systolic dysfunction in terms of severity , some of the patients show severe diastolic dysfunction out of proportion with systolic dysfunction.
Note : In the above patient it’s actually a fairly preserved systolic function but still has advanced diastolic dysfunction.

Grading of diastolic dysfunction .Image courtesy MM Redfield et al: JAMA 289:194, 2003. Note E:A >1.5 is
Final message
Relying on E:A ratio to diagnose diastolic dysfunction may appear amateurish for some of us .The rampant reporting of E>A for grade 1 diastolic dysfunction has made this parameter a “Doppler cliché”. But , the fact of the matter is, it does help us confirm severe (Grade 4) diastolic dysfunction when E stands tall and towering over an almost dwarfed A.
Clinical Implication
Please realise ,In patients with DCM when you find an A that is too diminutive in combination with a menacingly tall E , it may be prudent to raise diuretic dosage. It’s a sure signal for impending pulmonary edema.
Queued queries
Can DT and IVRT normalise with progressive diastolic dysfunction ?