I share my thoughts after going through this 85 page land mark document !

In whatever way I look at it ,It keeps both physicians and their patient population guessing in a confused sate regarding their cholesterol levels the treatment modalities !
It seems to revolve around a single point agenda, how to fit a single drug called statin in the scheme of things !
What if , a new drug comes and statin is proved not an angel in our fight against the evil of atheroscerosis !
Summary as I interpreted
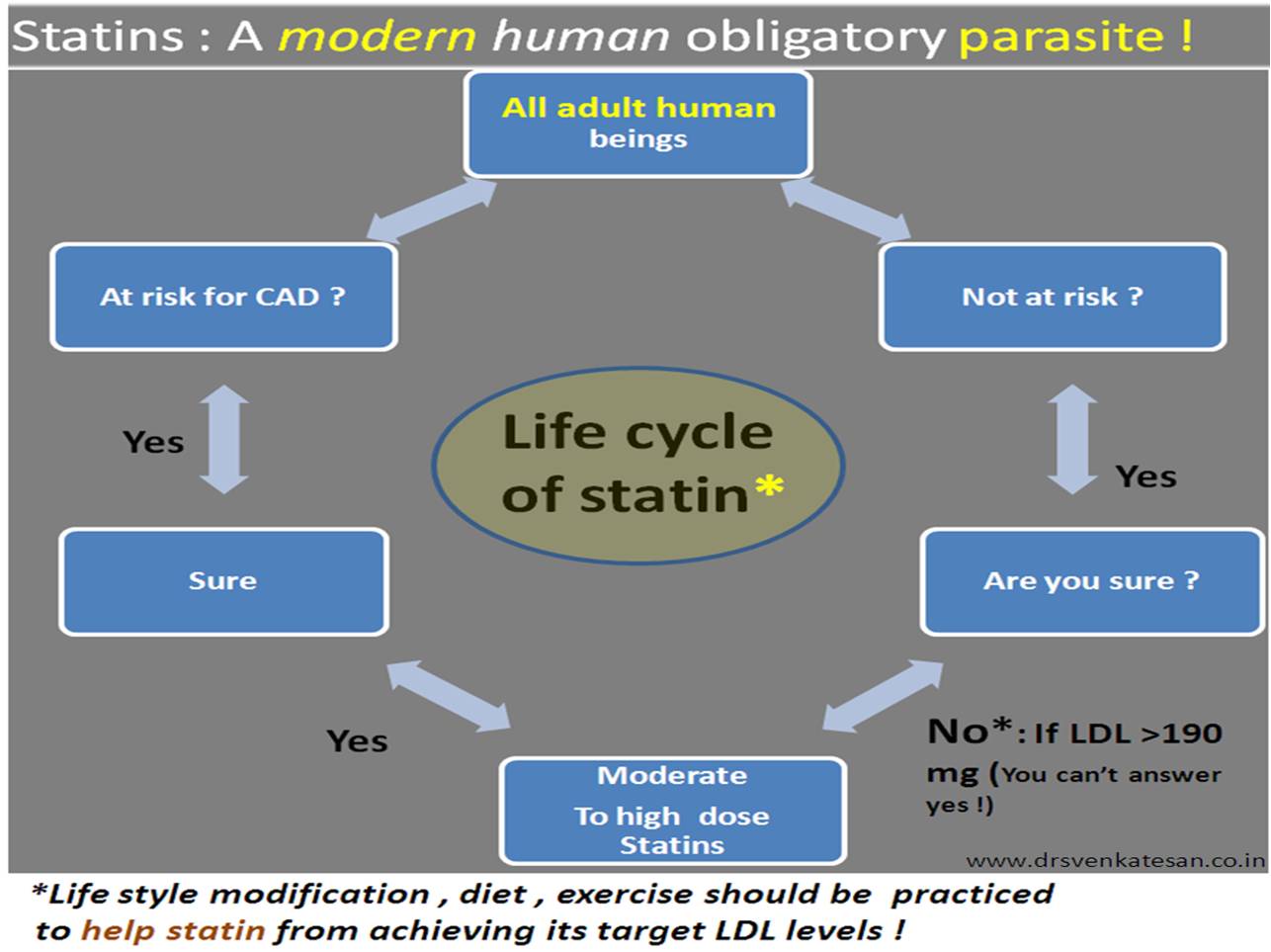
“All healthy and unhealthy human beings should ask only one question
whether they can some how benefit from taking statins ? “
If your answer is yes , administer the statin not in low dose but in moderately high dose ! (It appears there is little role for low intensity statins )
There is generally no need to to monitor the lipid levels as long as patient is comfortable.
Disclaimer : *Sorry , the Intention is not to hurt the hard work of a elite panel who toiled for years to bring this much awaited guidelines on lipids and atherosclerosis! but to express my view , biased though !)
A mini research
To confirm my assumption I did a curious word search in this 85 page document .
For words statin , diet and exercise
- Statin appeared 814 times
- Diet appeared 8 times
- and exercise just once in the entire document !
The importance of diet and body activity which are the primary determinant of serum lipid levels is mentioned in a cursory fashion in this global guideline meant to control the total cholesterol load and atherosclerosis of our population .
Meanwhile . a drug which acts in a physiological cell servicing metabolic path way in a complex fashion is glorified 814 times !Do you still think this post is is biased ?