This study was released in NEJM without much fanfare at the fag end of the last century, (rather the millennium) in 1999. Dr. Bertram Pitt and his team scripted this from the Department of Medicine, University of Michigan School of Medicine, Ann Arbor, USA. One can’t expect even in your dreams a study like this would be be done in the future.
This study tested PTCA vs with a single lipid lowering drug in terms of plaque regression. This conclusion is explicitly illustrated here, and the dramatically dissociated Kaplan and Myers would tell the whole story.
Can you name this trial that can withstand any period of time?
One clue : We do prescribe this drug every day and it beats angioplasty. Some of you may have got it right. Yes, It is the AVERT study: Atorvastatin versus revascularization treatment.(Ref 1) that dare to compare PTCA with a humble statin one to one, and we found the winner long long ago. This study also defined the bench mark for dosage of high intensity Atrovastatin at 80mg/per day.
Final message
I am sure, many of the current generation cardiologists may not know about this study and the conclusion might amuse them as well . The truth is , It deserves a 25-year anniversary celebration. Wishes and congratulations to Dr. Bertram Pitt.
Statins belong to a group of drugs, stolen and reengineered from the blueprint of natural Chinese red yeast rice (Monocoline K) in the late 1980s. The rest is the remarkable history in the pharma industry.
Statins directly interrupt the cholesterol synthesis by blocking HMG-CoA within the hepatocytes. It significantly lowers the LDL, fights human vascular atherosclerosis. It makes the plaque either regress, prevent progress, make it harder and in the process make them less vulnerable . There are innumerable studies that document the evidence. Statin has become a must-prescribe drug in any one with clinically established CAD or even in concealed CAD. Guidelines are available to prescribe statins various intensity, depending on the risk profile.
Which statin ?
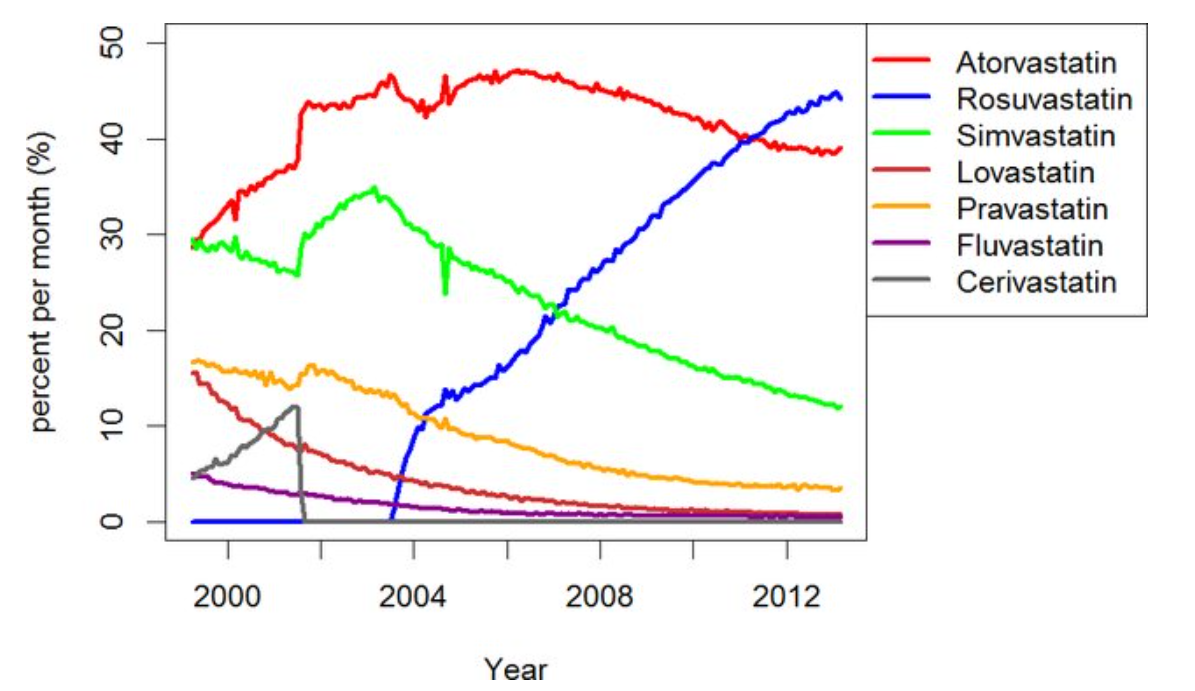
There has been a long list of statins. Many of them have retired from the ring .Currently, the fight is between Atorvastatin, a Rosuvastatin. Like Pepsi vs. Coke.
Note the graphic ,A meteoric rise of one drug since 2005 . (Can you guess the reason ?)
ATRORVA or ROSUVAWhich one should I choose ?
There is very little “one to one” comparison study between Rosuvastatin and Atorvastatin .The gap in the pros and cons are narrow. Following points are observed, without much dispute.
No one is dare enough to give strong verdict . Surprised to find one this month. BMJ has come out with a possible answer. It is called LODESTAR trial (Ref 1)
Mechanism of new onset diabetes with statins (REF 3)
It can be 7% with Rosuvastatin (less with Atorvastatin). We think, statins act primarily within the hepatocytes where cholesterol synthesis takes place, but they also have an eye on the pancreatic β-cells as well. It down-regulates GLUT-4 in adipocytes, and results in compromised insulin signalling. Furthermore, statins’ impact on epigenetics may also contribute to statin-induced T2DM via differential expression of microRNAs.
Mechanism of cataract with statins (Ref 2)
The cells lining that line the lens are dynamic and require cholesterol on a day-to-day basis. Statins inhibit proper epithelial cell development within the crystalline lens, where cholesterol biosynthesis is critical to maintain transparency and structure of the lens.
Final message
So, is it Atorvastatin or Rosuvastatin? It is left to you.
Mind you, “no statin at all” is the best option if circumstances and risk profile allows. Statins are never considered life-saving staple drugs in our fight with CAD and atherosclerosis. We, along with our scientists might may make you feel like that. Lipids can be controlled within desirable means exclusively with diet and exercise in most of the population* .
(*Forget about statins in the last 5000 years of known human existence, so many great people have lived a long and successful life in this world, without even knowing there is an organ called the heart that is responsible for the circulatory system)
In whatever way I look at it ,It keeps both physicians and their patient population guessing in a confused sate regarding their cholesterol levels the treatment modalities !
It seems to revolve around a single point agenda, how to fit a single drug called statin in the scheme of things !
What if , a new drug comes and statin is proved not an angel in our fight against the evil of atheroscerosis !
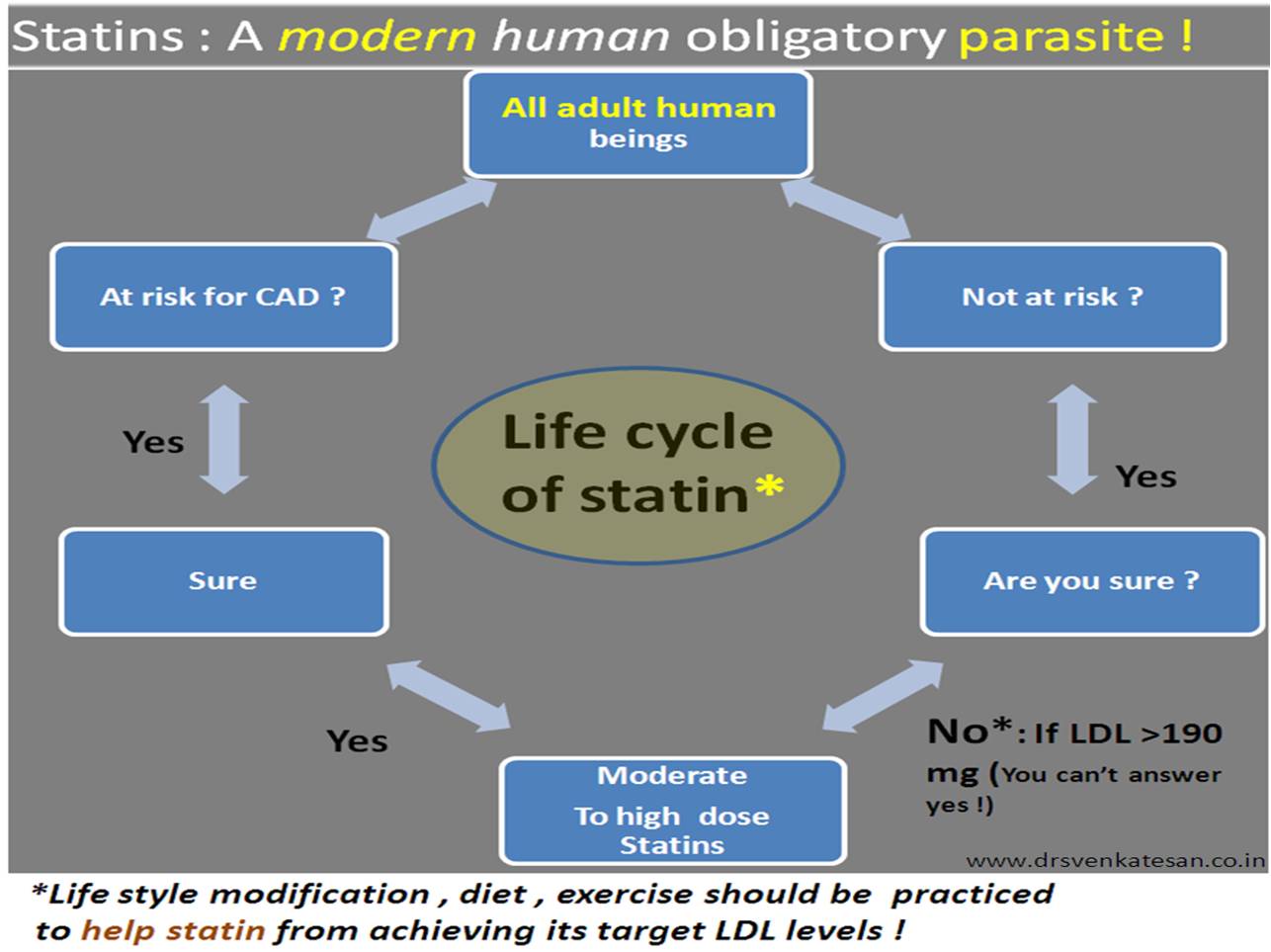
Summary as I interpreted
“All healthy and unhealthy human beings should ask only one question
whether they can some how benefit from taking statins ? “
If your answer is yes , administer the statin not in low dose but in moderately high dose ! (It appears there is little role for low intensity statins )
There is generally no need to to monitor the lipid levels as long as patient is comfortable.
Disclaimer : *Sorry , the Intention is not to hurt the hard work of a elite panel who toiled for years to bring this much awaited guidelines on lipids and atherosclerosis! but to express my view , biased though !)
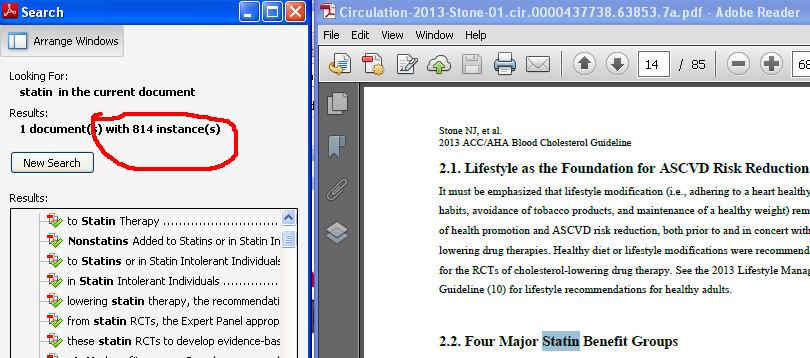
A mini research
To confirm my assumption I did a curious word search in this 85 page document .
For words statin , diet and exercise
Statin appeared 814 times
Diet appeared 8 times
and exercise just once in the entire document !
The importance of diet and body activity which are the primary determinant of serum lipid levels is mentioned in a cursory fashion in this global guideline meant to control the total cholesterol load and atherosclerosis of our population .
Meanwhile . a drug which acts in a physiological cell servicing metabolic path way in a complex fashion is glorified 814 times !Do you still think this post is is biased ?
Statins are projected to be the saviours of human race against the killer atherosclerosis .Now we have reached a stage soon , where every healthy individual may be administered this drug. There are consistent evidence for statins to reduce , retard , prevent progression of existing atheroscelorosis and possibly prevent future atherosclerosis.
This wonder drug acts by blocking the HMG COA enzyme a vital enzyme that regulates the lipid metabolism within the cells. It is made to appear as if , the God has created this enzyme with the only purpose for human suffering , by blocking this we expect all errors in lipid metabolism is corrected.
This enzyme is part of the house keeping system that is meant to service the human cellular lipid layers 24hrs a day. If it is impaired intentionally one can imagine the consequences. That’s what modern science is all about. Luckily God is kind enough the side effects of blocking this enzyme is seen only in minority. The myopathies that are classically described with statins are due to possible mitochondrial dysfunction .
As the debate still continues to find the optimal bottom levels of LDL , we have more worries , real world experiences have brought us a new issue namely the reduction of HDL with statins. While literature search on statins and HDL tell us there is marginal increase in HDL up to 10% the fact is there is marginal fall or significant fall in many of the patients .
How can this happen ? A huge difference between real world and trial world ?
* Brands shown not intentional
Readers are welcome to add their input on this question .
Treatment guidelines in cardiology practice are periodically published by ACC/AHA/ESC.These guidelines represent the current scientific practice. They are called some times as recommendations. Medical professionals tend to adhere to this guidelines whenever possible.They are not legally binding in most of the countries.In USA some states believe it, to be legally binding.
The problem with these guidelines are , they are classified as class 1 ,class 2 , class 3 recommendations.
Class 1, A drug , device or a procedure Is definitely useful and must be prescribed.
Class 3, A drug , device or a procedure Is not useful and should not be used .
Class 2*, A drug , device or a procedure may be useful or may be harmful , and hence may be used or may not be used . (Vaguest possible guideline!)
*Altered to convey the meaning
What are the guideline violations that can be sued in court of law ?
A person with established CAD who is not been prescribed a statin (Cholesterol lowering drug) can be sued straight away, even if the patient has no adverse outcome due to the nonprescription of that drug. The issue here is , the doctor has not prescribed a drug which has proven benefit .The law is clear on that .Most will agree that, the doctor is at fault , and he is never protected even by their colleagues .He can’t defend his action.
What are the medical errors that can never* be sued in court of law !
But the same doctor who opens up a totally occluding coronary artery in an asymptomatic patient(CTO -chronic total occlusion) and lands up in a complication and the patient dies. This could be major guideline violation as opening a CTO in an incidentally detected , asymptomatic patient is a class 3 recommendation. Neither the physician, patient , institution nor the regulatory authorities bother about this even though there is strong case for censure , in reality it never happens. Number of experts from leading hospitals do this procedure in live work shop all over the world with full media glare, It is an irony the same experts are only writing in their guidelines that these procedures should not be done inappropriately.
And this medical error ( Should we call it a crime if it is knowingly done ! ) keeps growing as the physician never feels guilty about it .
The message here is
A physician of a state of the art hospital, in a scientifically advanced country goes scott free and guilt free even if he openly violate the scientific guidelines and do a inappropriate procedure that result in a patient death. Mean while a small time physician in a remote place in the same country can be taken to task for not prescribing a officially recommended drug (By standard guidelines) .He will be labelled unscientific and unethical even if his non prescription , had not caused any untoward health outcome .
In short , in today’s modern medical practice
Even a ” Minor error of ommision” attracts guilt and perceived fear among the physicians. Meanwhile many of the ” Major errors of commission” done by professionals are rarely frowned upon and thus these mistakes continue to perpetuate !
*There should be a strong provision in medical law to address the issue of inappropriate procedures even if the procedure has not resulted any untoward effect to the patient.
Atherosclerosis is the number one killer of mankind .It involves all medium and large sized blood vessels.Any intima and media can be invaded by the disese process.Most common to involve are cerebral, carotid, coronary, aortic and it’s branches, renal, and peripheral arteries. But how pulmonary artery is missing in this list ? Is it really true (or) are we missing it ? One logical explanation is pulmonary circulation is a low pressure circulation and the maximum presssure is less than 30mmhg . This pressure may be insufficient to induce endothelial injury that predispose lipid mediated injury.
Other explanation could be a structural difference in the media and intima compared to aorta .But in patients with primary or secondary pulmonary hypertension where, inspite of PA pressure being high , still atherosclerotic changes is very uncommon . or Is it the Heath Edwards pulmonary vascular sclerosis grading reflects nothing but pulmonary atherosclero-thrombosis !
If this is true there could be a major role for HMG Coa reductase inhibitors in altering the natural course of pulmonary obstructive vascular disese . Statins might be tried in PPH a disese with no specific treatment !
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.