A 75-year-old male post CABG with severe LV dysfunction and ICD and dual-chamber pacer in situ presented with NSTEMI.
An angiogram revealed something, and he got this form of treatment. ? What is it?
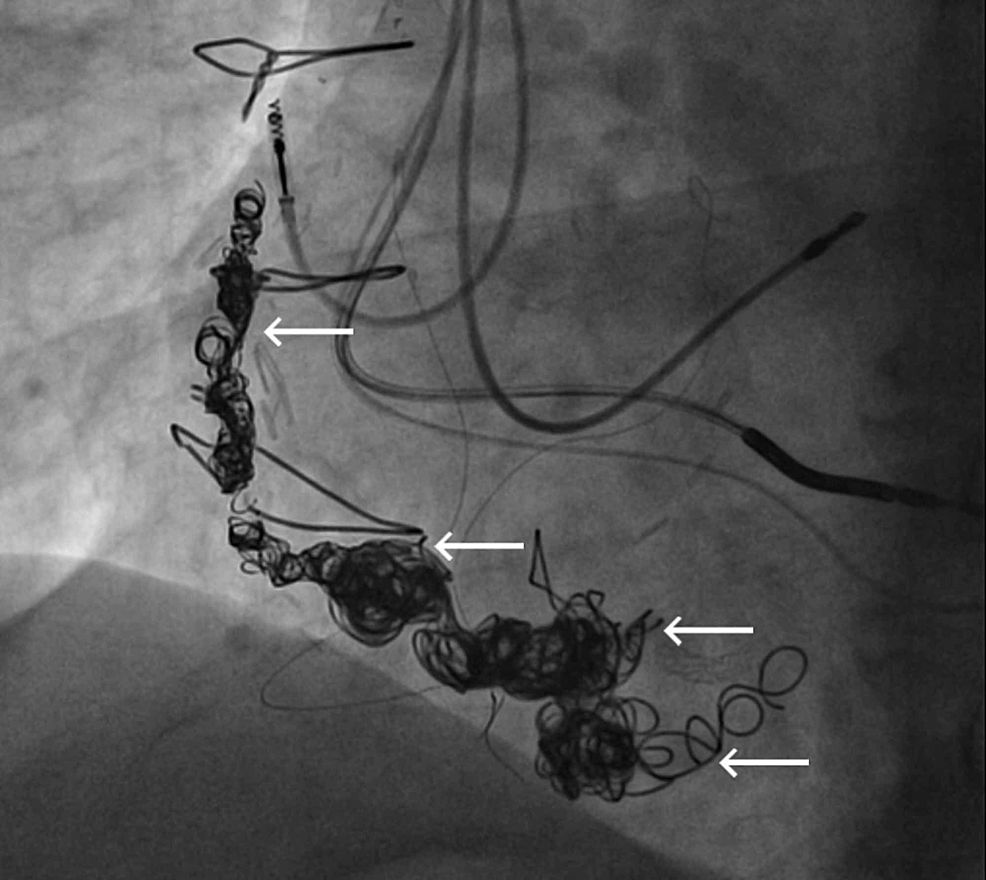
Features of SVG venous graft aneurysm
Graft aneurysm what are the risks?
- Thrombosis
- Recurrent ACS
- Rupture
Management
- Vascular plug
- Multiple coils (Does coil occlusion offer a permanent cure? I can’t think so )
- Covered stent
- None. No Intervention Just OAC & observe, follow up can be a good option and can beat all above three in many patients.
Reference
1.Ramirez FD, Hibbert B, Simard T, Pourdjabbar A, Wilson KR, Hibbert R, Kazmi M, Hawken S, Ruel M, Labinaz M, et al. Natural history and management of aortocoronary saphenous vein graft aneurysms: a systematic review of published cases. Circulation 2012;126:2248–2256.Crossref, Medline, Google Schola
2.Dieter RS, Patel AK, Yandow D, Pacanowski JP Jr, Bhattacharya A, Gimelli G, Kosolcharoen P, Russell D. Conservative vs. invasive treatment of aortocoronary saphenous vein graft aneurysms: treatment algorithm based upon a large series. Cardiovasc Surg 2003;11:507–513.Crossref, Medline, Google Scholar
3.Nolke L, McGovern E, Wood AE: Saphenous vein graft aneurysms; the true, false and ugly!. Interact Cardiovasc Thorac Surg. 2004, 3:631-633. 10.1016/j.icvts.2004.07.011