One of oldest hospital in the world , is now an UNICEF heritage site. Santa Creu , Sant Pau original hospital built in 1400 AD rebuilt in 1900 by Catalonian modern architect Montaner.

Architecture by Lluís Domènech i Montaner


 Reference
Reference
Posted in Uncategorized, tagged heritage hospitals, histroy of medicine, sant pau hospital unicef barcelona on September 30, 2014| Leave a Comment »
One of oldest hospital in the world , is now an UNICEF heritage site. Santa Creu , Sant Pau original hospital built in 1400 AD rebuilt in 1900 by Catalonian modern architect Montaner.
Architecture by Lluís Domènech i Montaner
Reference
Posted in echocardiography, tagged tvi, tvi by echo, tvi in doppler, tvi unit is cm, What is the unit for TVI ? Echocardiography, what is time velocity integral on September 30, 2014|
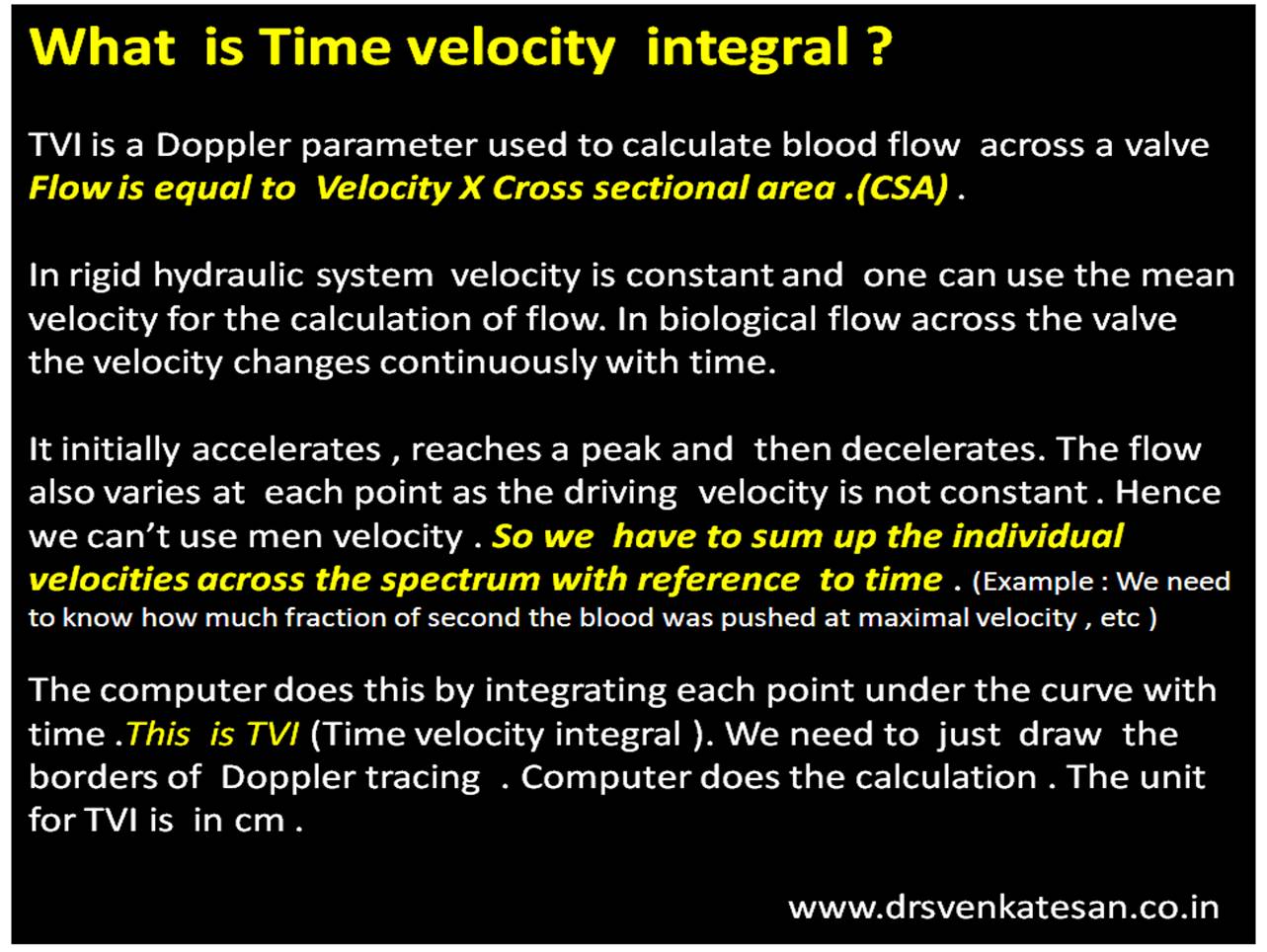
TVI (or VTI) is a hemo-dynamic echo parameter measured from Doppler spectrum across the valves ,usually in the outflow.This parameter is used to calculate cardiac output .VTI times the cross sectional area gives the stroke volume.
A correction: TVI is multiplication of velocity into time not division as suggested in the cartoon
Time velocity Integral
Summary
*VTI is a Doppler parameter described in cm , it can be referred to as Stroke distance.This stroke distance when multiplied by valve area gives the stroke volume from LV/RV (or flow volume across AV valves or through any conduit)
Posted in Uncategorized on September 28, 2014| Leave a Comment »
One of the hottest debate in the recent world cardiology forum in Barcelona WSC 2014 , was about how to tackle incidentally detected non IRA lesions during primary PCI.
So far , the dictum is , one should not meddle the non culprit lesions unless demanded by hemodynamic instabilty .The next option is to do a staged PCI for these lesions. (Few days later). or just forget about these lesions unless they are critical.
Now new studies are appearing that suggest doing all “do-able” lesions must be stented in one go ! This is obviously inviting trouble .The worry is not in the concept but with the dubious track record , fragile guidelines and potential ethical debacle of the cardiology community !
Stent “As you want and as you please” has already invaded our mindset in the chronic coronary scenario. Now in 2014 , we want more freedom in acute coronary syndrome as well ! We can’t ask for a referee less game of soccer !
We clearly know coronary arteries are to be respected and do not deserve indiscriminate stenting especially in ACS where the early hazard is more.
A recent story which I heard was a height of futility . A semi experienced cardiologist in the suburbs of a big southern Indian city , opened successfully a LAD which was the IRA and subsequently caused acute LCX STEMI , while trying to tackle an insignificant non culprit lesion due to procedural mishap ! (Some suggested migration of LAD thrombus !)
What a pity , when we are supposed to arrest the culprit, in reality it is simply chased down to another territory !
Here comes unique advantage of thrombolysis , you need not locate the culprit artery the drug chases it wherever it is , even if they are multiple ! Read in this link :
Final message
We call it as fate when thrombus suddenly occlude a coronary artery and the IRA becomes a culprit . We need not compete with fate and end up creating potential new culprits.Let the sixth sense prevail over the five .Use judicious discretion when trying to stent muti-vessel CAD during PCI. Please realise ,the concept of multivessel stenting during pPCI is not wrong . How we interpret is the issue !
There is no excuse to indulge as you like , simply because your intentions are good !
Posted in Uncategorized, tagged happiness quote, happy doctor on September 25, 2014|
Posted in Cardiology - Clinical, Cardiology -Clinical signs, Cardiology -Mechnisms of disease, cardiology- coronary care, Clinical cardiology, tagged angina vs infarct, difference between stemi and nstemi, epicardial angina vs endocardail angina, heberden angina, how is chest pain different between nstemi and stemi ?, rca vs lad angina on September 24, 2014| Leave a Comment »
When a patient comes with angina at rest , it could mean two things .Either a STEMI or an NSTEMI .This , we can diagnose only after seeing the ECG .
Can we differentiate these two by the character of chest pain alone ?
Very tough task isn’t ? But there are some definite clues .
Infarct pain
Unstable angina
Mechanism of the difference : Epicardial vs Endocardial angina
The pain of UA is due to subtotal occlusion and endocardial ischemia , while STEMI is sudden total occlusion and the resultant transmural ischemia . In STEMI epicardial surface is always involved (Which lifts the ST segment in ECG .).We know epicardium is same as visceral layer of pericardium which is well innervated .Hence pain of STEMI acquires more of somatic character than a predominately visceral type pain that occurs with UA/NSTEMI where epicardial ischemia is absent.
Clinical importance
The demarcation between unstable angina and Infarct pain becomes vital when we calculate the time window for thrombolysing STEMI .Many of them have a phase of pre infarction angina which is a type of unstable angina. If we mistake it for Infarct pain then one may falsely calculate a prolonged time window and deny re-perfusion therapy.
Post -amble
It is tricky issue to differentiate the chest pain of STEMI and NSTEMI .A significant overlap can occur in real coronary care scenario . We know chest pain that occurs in both pre and post infarct phase is considered as unstable angina .(With infarct pain sandwiched between them!) Hence differentiating them may even be termed as futile.
Still,clinical cardiology can be made fascinating by indulging in such exercise !
Posted in Uncategorized, tagged Mechanis m of tall T in hyperacute MI stemi on September 10, 2014| 1 Comment »
Most of my students were struggling to answer this seemingly simple question . I realised later it is indeed a difficult one !

Some thoughts
Tall T waves are observed in very early phase of STEMI .(Within 30 minutes ?) What is the mechanism ? Since ST shifts occur little later than T elevation ( considerable overlap may occur) it may not be related to current of Injury.It is an inherent alteration in the T wave genesis .T wave is inscribed when rapid phase 3 K+ efflux happen (Mainly by Iks and also IKr )
What is the effect of ischemia on K + channels ?
No uniform answer.(Blocks, stimulates, irritates, Bi-phasic, variable ?)
There are 6 important K channels in every cardiac myocyte adding to the complexity.
Does the Ischemic cells leaks potassium or accumulates it ?
Though It does both , predominantly it should leak .If it’s leaking there is local extracellular hyperkalemia . Is that the explanation for tall T waves ?
What is the influence of QT interval on T wave morphology ?
Long QT as occurs in hypokalemia pulls the T down and it may even invert it. .Short QT tends to push it up as in ERS .The effect of ischemia on QT interval is again unpredictable.Further regional and remote ischemia in a given patient can alter this.
Once the ST begins to elevate the T waves losses it power to grow tall .It only can regress. I think this is the time the QT is sort of prolongs .
Effect of reperfusion on T waves
The tall T tend to regress as some form perfusion takes place as K+ Is pushed back into the cells or flushed away from the vicinity.
The dynamic nature of reperfusion makes the behavior of T wave amplitude further complex. But one thing is certain , a well perfused IRA is associated with inverted T wave which we call it as completion of the process of evolution of MI .
Finally and most importantly this hyper acute T phase is not a constant phenomenon. In fact it is uncommon in persons who have baseline T inversion .After analysing many things we are back to the original state of ignorance .
Summary
Researchers with intra-myocardial micro electrodes try to decode the mysteries in electrophysiology . Still there is a huge disconnect between clinicians and physiologists.
In simple terms I would believe the mechanism of ischemic tall T waves are almost similar to renal hyperkalemia. (A local , transient extracellular k + excess ) The base of the T waves are not narrow and tented as in CKD because some degree of ST elevation (that always is expected ) widens the base of T wave. Further ,the prolonged QT interval in renal hyperkalemia stretches the QT and encroach the base of the T wave to the left making it appear narrow.
A simplest version for students
Tall T waves are due to transient local extra cellular hyperkalemia , when K + leaks due to cellular Ischemia.
Caution: This is a superficial scientific attempt .I need inputs from more scientific brains and electrophysiologists.
Read further
Posted in Public Health, Public health issues, tagged better world, brain death defintion, cadaver organ sharing india, ethical medicine, future of man kind, heart transplantation in India, humane medicine, kidney transplantation india, net work for organ sharing, organ transplant act india, role of who health, sucide and cardiology, sucide victims as heart donors, unos, who, world health issues on September 7, 2014| Leave a Comment »
I got this alert from World health organisation yesterday .Click over the image to read more .

Why should a cardiologist affected about this ?
When we are fighting in cath lab day in night day out to extinguish the myocardial fire set by coronary thrombosis and the resultant STEMI . . . the solemn attempt to salvage whatever myocardial cells we can !
See . . . what is happening elsewhere every 40 seconds a healthy heart in toto is executed by weak minds !
What should the WHO do ?
Just publish these data and forget . No,they should organise the world leaders to take a resolve !
Either , we should prevent these unnatural deaths or else we should have world organ net work. Why can’t we use these weak hearts for those courageous men and women who lose their life daily with end stage cardiomyopathy who long for living !
Is this possible ?
Why not ? Ain’t the world leaders group together periodically to impose a sanction or bomb other countries for personal reasons !

Posted in Public health issues, tagged asd vsd pda, bore-well deaths in India, congenital heart disease, hippocrates oath, hole in the heart, hole in the heart and hole in the road, Indian association of pediatrics iap, public health issues, safety issues for children, who child safety on September 6, 2014| Leave a Comment »
I stumbled upon a TV reality show where a mother of a child was crying inconsolably ,whom she lost when it fell into a open bore-well pit .She was blaming it as her fate and the hole was sent by Lord Yama (God of death )
I just got curious ! This article was written in a flash.
I used to get questions from anxious parents of children with holes in the heart .(Asymptomatic small VSDs or ASDs who come for periodic echo-cardiograms) .I reassure and convey the message , most of these holes are tiny and will close automatically and they need not worry.Even if it doesn’t, it poses little problem.
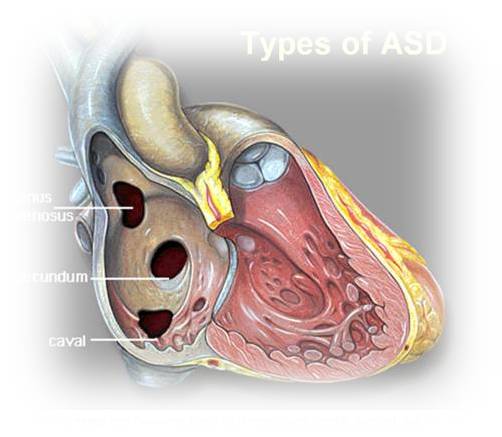
But .after watching that haunting TV show, I have started to warn the parents that holes in the heart may not be that dangerous but be wary of holes in the roads and unclosed bore wells in our country !
Every single parent was amused with my statement ! Some how it appeared sense to me !
I made a mini google research. It is estimated thousands of bore-wells are dug every day and kept open in allover the country side .It is like live land mines . Some press reports suggest at least one child dies in India every day due to uncovered bore-wells and man holes ! (May be really true !)
The following are some of the samples.
One

One more

Two
You can understand the gravity of the problem , one engineer has devised a special child retrieval Robot for such accidents.

Three
A news report in Times of India .What shall we do about these ?
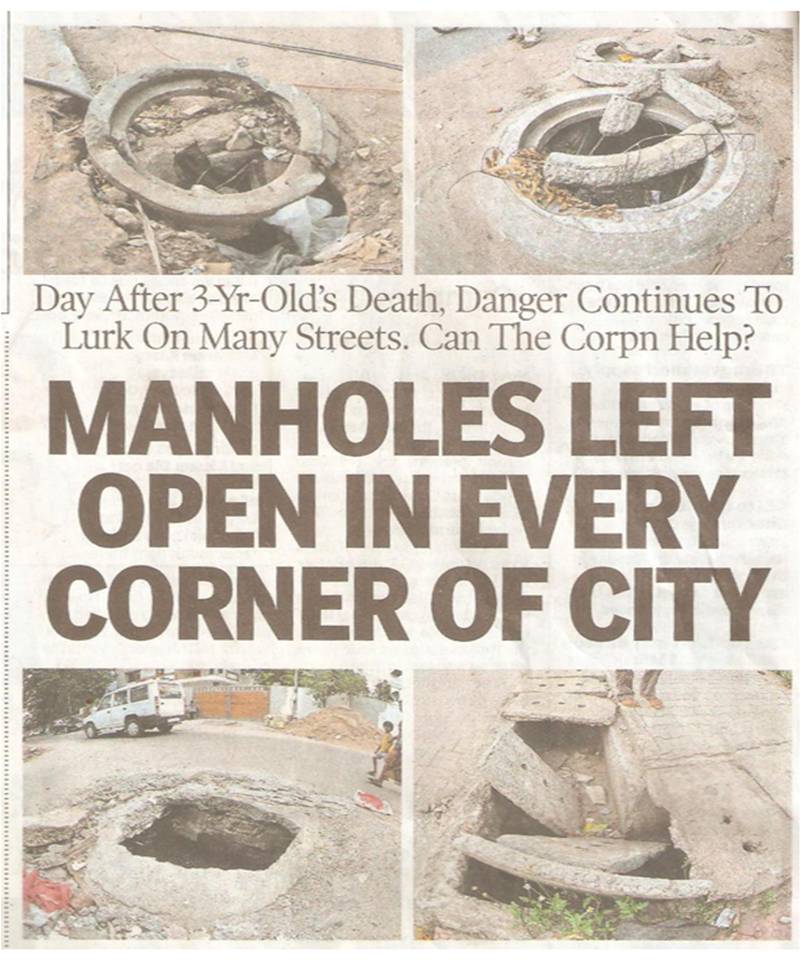
It is a horrific truth in this civilised world .Nature creates holes in the heart due to defective gene in some . It appears less dangerous to me. After all a hole in the heart threatens only one life,while a hole in the road kills many people.
As a cardiologist , I am saying this with anguish as our team along with surgeons work over time to close intra-cardiac holes with device , the holes in the road are often callously kept open forming death traps for our children .The men responsible for such things deserves no pardon.
The story is never ending . . .

Posted in cardiac resynchronisation, Cardiology - Electrophysiology -Pacemaker, tagged crt vs icd, when should i use combo device ?, when should i use crt and icd ? on September 5, 2014| 1 Comment »
CRT is done for advanced heart failure to improve exercise capacity and hence the quality of life .It does not do any thing significant in prolonging life .ICD is again implanted in advanced LV dysfunction with either documented VT/VF or patients who are at propensity for VT .It has dramatic benefit in preventing sudden cardiac death.
Both CRT and ICD has some overlapping indication in cardiac failure. Attention young cardiologists, please realise among these two the value of ICD is many many fold higher than CRT.This fact is rarely discussed and disseminated.
True benefits of CRT is realised only when it is combined with ICD.
Summary
*Except in patient with degenerative complete heart block , both ventricles are paced the term Bi-Vi pacing is used instead of CRT.Since LV function is normal here , there is no de-synchrony in the first place .The synchronised BIVI pacing is meant to prevent future heart failure
Final message
Always use a combo device in advanced symptomatic heart failure which is refractory to medical therapy.
After all , there need to be a life in the first place so that we can improve it . ICD ensures life while CRT tries to improve it.