AVR plus MVR commonly refered to as DVR is a path breaking cardiac surgery in patients with combined valvular heart disease. Still, it carries considerable mortabidity, if not done with high degree of expetise and standards . Apart from technical perfection, an inherent issue exist that might affect long term Impact.
Here is lateral view of X – ray chest showing a DVR.
Note :The green ring denotes the mandatory gap to avoid metal clash ( a missing biological link) in the Aorto mitral continuity
Final message
What will happen to the native anatomical and physiological functional unit of Aorto-mitral continuity after DVR? Will LV inflow encroach the LV outflow or vice versa? These questions are less often asked. In the process, we often ignore a concept called Aortic-mitral coupling or inter-dependence.
Stents have become essential coronary jewelry in global CAD care. The usage of these glamorous metals inside the human heart has crossed many millions, and aiming for a billion. Obviously, when used on such a large scale un-toward events are not an exception.
Stent migration
While the complication list of coronary stenting hangs long, fortunately, stent migration is a rare event. , Though, early geographical miss is common during deployment, these episodes don’t come under stent migration. Stent dislodgement during the procedure is a more common technical defect.If not recognized it may be wrongly labeled as late migration Exaggerated longitudinal shortening sometimes mimics migration.
Minor stent skids or mini migrations in cath labs are acceptable, distant and wayward migration to dangerous zones can be problematic.
True migration may be defined as a stent moving away from the target zone in the short or long term from its original location. It is useful and can be further divided with reference to time like peri procedural, short term, and late. Though it is generally thought to be rare true Incidence is not known. (Colkesen AY, . Int Heart J. 2007;48(2):129–136.)
Mechanism
It is not always easy to find the reason for migration. Many of the following factors could operate
It is tempting to blame the technique, inappropriate size (small for the lumen), and lack of imaging whenever migration occurs.(Very often one of them is true)
Metallurgically, it is the radial strength that keeps a stent in its original place. if for some reason this force is lost there is potential for migration of the stent. In this context, there is a link between stent fracture, injury infection, and migration of the stent.
A vasospastic coronary artery holding the stent tight and later releasing the grip is a rare possibility.
Liberal use of vasodilators like nitroglycerine might contribute. A case report from Pakistan suggests this possibility Murat Celik, Pak J Med Sci. 2013
The coronary artery is not a static tube so is the stent . the artery can milk out foreign bodies if it wishes. Fortunately, it doesn’t. Instead, it reacts with metal and initiates an inflammatory and rejection process that may ultimately end up as infective aneurysm and the stent can migrate outwards or extraluminal into the aneurysm sac. We realize, this is more common than other forms of migration.
Retrograde migration is a baffling complication as in the following case.
A LAD stent migrates retrogradely into the aortic root crossing the left main ostium. Image source and courtesy Hilary Bews and others, Coronary stent on the move, European Heart Journal – Case Reports, Volume 5, Issue 12, December 2021, ytab511, https://doi.org/10.1093/ehjcr/ytab511
Implication
Stent migration can be totally unrecognized by many, while could end with a dramatic clinical event depending upon the extent and location of migration.
Though it is a sort of crisis for cardiologists, very often patients are asymptomatic and comfortable in spite of migration. (After all, it is the same pro-thrombotic foreign body even if it is present in its original place, is it not ?) Minor migration or embolization to safe zones need not require any intervention.
What should we do if leaving alone is not an option?
Crossing the stent and deploying it again or trapping or crushing it with another stent or retrieval are various options. Surgery is the last resort if the migrated stent is compromising blood flow critically.
Stent migration: A mini ethical crisis
Should we inform the patient about this adverse event?
Never hide any info from your patient about his or her health. It may amount to serious negligence. Sorry, I beg to differ*. If we really feel, it is a safe migration, and if the patient’s (& relatives) anxiety is too high, principles of practice of medicine can be selectively put on hold, for the overall benefit of the patient. (Of course, legal requirements are to be fulfilled by documenting the event in a complex manner as the lawyers do )
*Once you inform the patient, the option of leaving it unattended is a Herculean task even if it’s benign migration. (at least in our country) We have had long debates about this. Once upon a time, we had a stent that got dislodged and lost in circulation, and after long times of screening, there was a suggestion of a stent in the pelvic branches of the iliac artery. I will leave to your imagination, what we did for that patient.
Final message
Stents have conquered our profession and it is a life-sustaining device for both patients and cardiologists. Along with it, we have percutaneous valves, wires ,plugs, disc conduits, ICDs etc, Welcome to the big world of vascular foreign bodies. We are supposed to get optimally trained to keep all this stuff within the circulatory system smoothly running. If you look in that perspective, stent migration may be considered a minuscule untoward event. This doesn’t mean we can take this entity casually. We need to be familiar with its true incidence, mechanisms, potential solutions, and preventive strategies.
Reference
1.Bews and others, Coronary stent on the move, European Heart Journal – Case Reports, Volume 5, Issue 12, December 2021, ytab511, https://doi.org/10.1093/ehjcr/ytab511
2.Kasegaonkar AM, Chudgar P, Kamat N, Burkule N, Dhareshwar J, Dalal A. Delayed Presentation of Intracoronary Stent Migration in Pericardial Space: Role of Imaging. Indian Journal of Clinical Cardiology. 2022;3(4):209-210. doi:10.1177/26324636221087108
I think this child underwent successful surgical correction.
What is the mechanism of angina in coronary AV fistula ?
Coronary steal is easy explanation. But, very few of them develop functional Ischemia even at exertion. Why ? Size of fistula. dainage site, complex tortuous tracts, associated microvascular obstruction, contribute more.
Reference
Angelini P. Functionally significant versus intriguingly different coronary artery anatomy: anatomo-clinical correlations in coronary anomalies. G Ital Cardiol. 1999;29(6):607–615. [PubMed] [Google Scholar]
Cath lab nightmares may be a cliche word for all of us. Still, It has become a mandatory topic in any cardiology conferences and live workshops. These sessions are always popular and crowded as Interventional cardiologists are eager to get tips from other experts, on what to and what not to do in the cath lab in crisis situations. While stuck in an unexpected problem, these tips really help us come out of this, with shared expertise, presence of mind, skills, innovation, etc.
I asked them, what can be done about this ? “Nothing much” was the unanimous response
Final message
To end on a positive note, nothing is Impossible. Let us first start feeling this moral nightmare, and quell it at its origin. Fortunately, this doesn’t need sophisticated hardware. All we require is a little bit of righteous & peaceful application of mind in the way we learn and practice science.
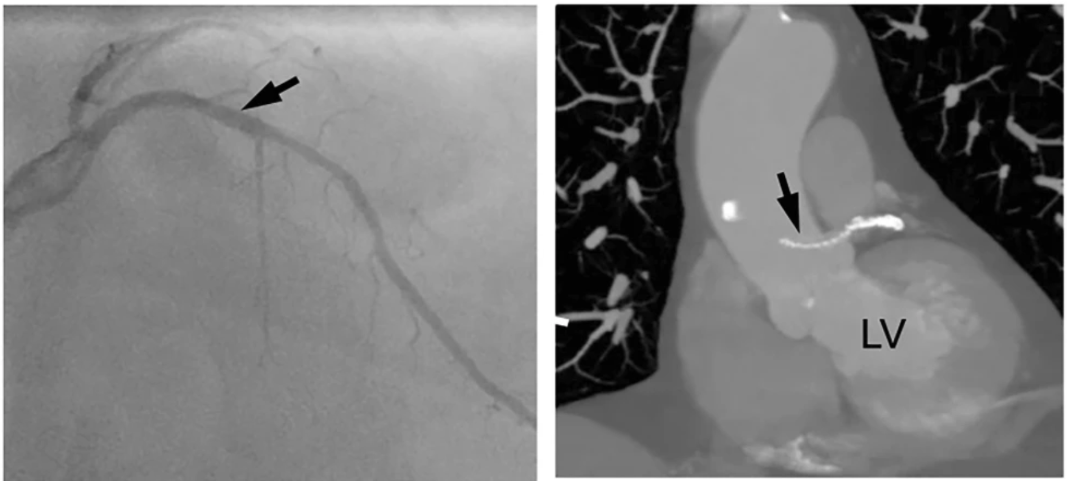
Whenever possible ,before doing a coronary revascularisation procedure , check twice the segments you try to perfuse is really short of blood supply and truly needs the procedure. Don’t ever waste your resources and try to blood-feed the dead myocardium. It’ can never be awakened !
Pragmatic science
I was conversing with my colleague recently , who has grown into suave , Interventional cardiologist with a huge academic & societal repute .He owns a personal cathlab and planning to get one more.
I learnt a non-academic reality lesson from him .
When planning myocardial revasascularisation, apart from myocardial viablity status, there is one more viability issue which is done in the account books of finance mangers across big hospitals. Its Cath lab viablity. Trust me, he used exactly the same word ! He went on to explain in detail , how, every day there must be a minimum number of procedures to keep the machine alive. Which is under the eagle eyes of the guys who funded the state of the art lab !
“So, what do you say,I asked him ?”
He was frank enough to admit, he felt always happy when he is able to convert angiograms into angioplasties.He went on to add , the Ideal CAG-PCI conversion ration should be atleast 3:1 or more.
“Whenver I hear such genuine statments from real world people , it pains, as it tends to confirm my assumptions ”
Final message
I am wondering with all my lost wisdom. Why should any cardiologist after 30 years of training, fight for cath lab viablity , and get into a conflict with the very organ they are supposed to care and protect.
When did we become so Inferior beings & fight for the survival of these life less machines ?
Meanwhile, major text books , has un-intentionally facilitated this academic deciet .They have largely taken away the sting out of the snake . Myocardial viablity , hibernating, stunned myocardium , are rarely given importance nowadays and made it appear taboo concepts,in cardiology academia.
Postamble.
Will be extremely happy if what is portrayed in this post is not really true.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.