Management of recurrent ventricular tachycardia has developed a lot in recent times. Anti-arrhythmic drugs(AADs) were a cornerstone for most recurrent and refractory VTs till recently. Surgeries including CABG, repair of the aneurysm, and subendocardial resection has helped to control many post-MI ischemic VTs. Soon they became obsolete. Realistically, PCIs had little impact on post-MI VT for some unknown reasons. However, with the advent of ICDs and RF, ablation, a new dimension is added to this field.
ICDs, though an attractive device, don’t prevent a VT but vow to nullify the consequence of VT. This is problematic. ICDs in spite of their ability to prevent SCD effectively, it has little say in preventing non-sudden deaths of in any form of cardiomyopathy. (In fact, there is some evidence ICDs might increase myocardial damage with inappropriate shocks )
Hence, RF ablation can be called as true curative therapy by extinguishing hot spots of VT genesis. Still, we need to understand ablation is technically creating new dead myocardium (in alreadly damaged myocardium) and hence, can’t avoid a consequence. More importantly, ablation as a modality is technically more demanding. We have accumulated huge experience with the help of electro-anatomic imaging and cutting-edge hardware in the last few decades. Still, we find it difficult to zero in the target area of RF ablation, with all available techniques of mapping (Activation, substrate, entrainment, and pace mapping) The reason is, VT circuits can be really complex ones. Not only different loops but also it can travel deep into the myocardium (Intramural or epicardial) making a single approach endocardial often futile. Success rates vary between 60 -70% (Some may claim 90 +)
This post wants the young fellows to take on this fundamental issue and learn in-depth about the arrhythmia circuit.(Get Inspired by Dr. Samuvel Asirwatham of Mayo clinic work )
What is the best site to ablate ventricular tachycardia?

- Exit point
- Central isthmus
- Entrance
- Inner loop
- Outer loop
- Though logic would tell us we can intercept an arrhythmia by ablating anywhere in the circuit. But the issue here is we need to permanently ablate it. not just interrupting.
- The best site to ablate is the exit point or entry point. Maybe isthmus. I am not really sure. But, one thing is clear, the outer and inner loops are not important. Further, live tissues are the culprits and not the scars and infarcted zones.
- One more possible answer is to try to ablate all (or maximum) points in the circuits.
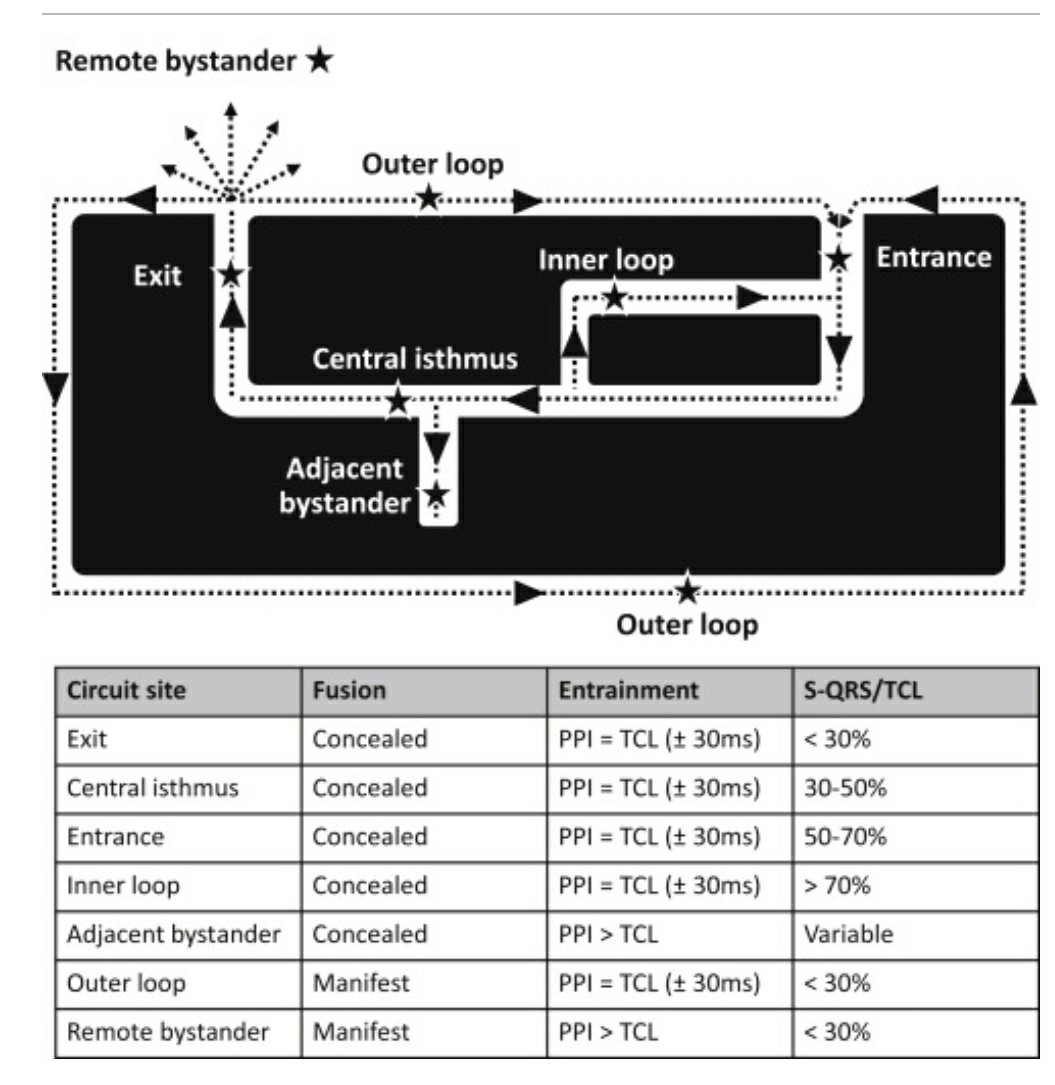
How to identify entry points and exit points?
Not a simple answer .EPs apply their life experience to do that, assisted by technology. Not everyone who has a Carto -GPS can do that.
One simple answer for the fellows is, in entrainment mapping, critical sites can be somewhat arbitrarily labeled as exit, central isthmus, or entrance on the basis of the Stimulus-QRS interval relationship to the TCL. Exit sites will show an S-QRS interval < 30% TCL (QRS onset shortly after pacing), central isthmuses will show an S-QRS interval of 30% to 50% TCL (some delay in QRS onset after pacing), and entrance sites will show an S-QRS interval of 50% to 70% TCL

Ruairidh Martin et all Circulation: Arrhythmia and Electrophysiology. 2018;11:e006569
Final message
Key to the successful ablation of VT is the accuracy in choosing the target site. Locating the target is meaningless if we can’t reach that site. Reaching the site is again futile unless we are able to deliver adequate burning or icing with sufficient contact.
Meanwhile, AADs can never be ignored in spite of the apparent side effects, for the simple reason they reach the VT circuits without any fuss. The Pharma industry has almost lost its interest in AAD research and the hyper-talented EP guys are squarely responsible for this unintended consequence.
Future directions
RF energy modification and newer catheter designs will help. While cryoablation shows a promising advantage over RF, it is still to prove its sustained efficiency. Meanwhile, other ablation modes are being tried. Transvascular ethanol ablation and stereotactic radio ablation have both shown promise for arrhythmias that fail other ablation strategies.
Some more questions
- What is the difference between arrhythmia focus of origin and entry point?
- Once the VT is set in, what is the relevance of its origin?
Reference
One of the very good reviews on the topic.
1.Gustavo S. Guandalini, Jackson J. Liang, Francis E. Marchlinski, Ventricular Tachycardia Ablation: Past, Present, and Future Perspectives,
JACC: Clinical Electrophysiology, Volume 5, Issue 12, 2019, 1363-1383,
2;,W.G. Stevenson, H. Khan, P. Sager, et al. Identification of reentry circuit sites during catheter mapping and radiofrequency ablation of ventricular tachycardia late after myocardial infarction Circulation, 88 (1993), pp. 1647-1670
3.M.E. Josephson, L.N. Horowitz, H.L. Waxman, et al.Sustained ventricular tachycardia: role of the 12-lead electrocardiogram in localizing site of origin Circulation, 64 (1981), pp. 257-272
Read Full Post »