Current generation doctors are gifted, can be immensely proud to practice medicine with cutting-edge technologies and advanced medical therapies .Today is the official doctors day in India, in honoring one of most great physician of our times Dr.B.C.Roy on his birth day.
Who celebrates Doctors’ day and for what ?
Sharing here , one of the deeply reflective article about, reality of being a doctor today. Published in today’s Hindu, (July1 2025)India’s National New paper, Opinion Column by Dr C. Aarvinda . It is a 6 minute read, must for all those who truly love our profession.
Courtesy : Dr.C.Aravinda MD, Assistant Professor of community medicine. Thanjavur medical college. Tamil Nadu .India.
While the profession is glorified at every level, there seems to be little to celebrate at a personal level. The same public who celebrate doctor’s day , become a mute witnesses to innumerable attacks unleashed on them on a day-to-day basis across the country. It is a sad truth the medical profession has been hijacked, far away from its original intended destination by both visible and Invisible forces. Many honest, hardworking, and humble doctors are compelled to traverse a turbulent moral landscape.
Final message
Doctors’ day celebration is meant for whom? Realistically, it is the occasion for patients who respect and show love to their healers. The whole idea got distorted in recent times. Definitely, it is not meant for pride hunting and forcible Intrusion by the industry , into the noble profession.
A patient who had a PCI some time back , asked me in one of his recent visit.
Doctor what is microvascular endothelial dysfunction and erosison ? Am I at risk of developing it ?
What am I supposed to answer ? Yes, I some how managed .” Don’t worry , it is a complex biological phenomenon. you need not go deeper into that. Take medicines regularly” He wasn’t happy with my answer is a different story.
A simple tip for peace of mind … for the modern patient
If the current generations of patients , equipped with hyper-knowledge engines, insist to understand 100% about their illness, imagine the consequences to the global healing system ,that has so many ground level issues to bother about.
Oneunofficial estimate from an elite , professional academic chatterbox of medicine suggests that the knowledge base with which doctors diagnose, treat, and understand the diseases they tackle, is at best 15%. Pateints need not be thankful , but atleast understand we are for working around with 85% ignorance, and still tries to bring out the best. I am sure this is a fact, no one can disagree ,regardless of the presence or absence of evidence to support it.
Final message
It might appear fair if someone argues blind faith in a trusted physician or hospital could end up as unscientific or unethical. But,what they fail to realize is, sciences’ blindness can be much darker, especially when it comes to the outcome of treatment and prognosis.
Yes sir, It was acute decompensated LV failure, Patient was in impending pulmonary edema. In fact, he developed. He is fine now,
How did he come around? He was too sick I thought.
“Just pushed 60 mg Frusemide IV, luckily he also had good BP, so with an infusion of NTG, titrated Carvedilol a little bit, he came out nicely. I guess it is Ischemic DCM”.
“Good, You have done a nice job”
“Don’t make me embarrassed sir. It is such a routine in our ER.
To make him curious, I asked “Which drug do you think that saved him”?
“Obviously, Frusemide sir. He was frothing out. I thought he will require a ventilator. It was a matter of 20 minutes, sort of flushing out 500 ml lung fluid through the urine”.
“No, you are wrong. As a professor and cardiologist, I need to tell you this. Diuretics never save lives heart failure.
Sir, I guess, you are not kidding. Does this statement apply to acute heart failure? We have saved 100s of lives with Frusemide, both in acute, acute on chronic, and even in chronic cardiac failures with metolazone.
Hmmm, I agree with you my dear student, Frusemide has saved not hundreds but lakhs of lives in the past decades in all forms of heart failure. It continues to do this fabulous job even now. But, don’t say it in exams or scientific forums. It has no evidence to show survival benefits. You can’t credit a drug without evidence. Also realize, saving lives by unscientific means by a cheap generic is not something to boast upon. We need the blessings of RCTs, or Kaplans Mayer curves, or Forrest blobbograms. Unfortunately . that is the current principle of practice of medicine.
But sir, who is preventing whom, to do such studies. Why they are not comparing diuretics one to one with these modern drugs of inotropes, calcium modulators, or SGLTis, etc?
I am not sure. My guess is, there are no good friends in the cardiac failure research community for this old warrior drug.
Loop diuretics
Till 1960s, toxic mercurial compunds was the only option to drain water in heart failures. The Invention of Na+/K+ /Cl channel blocker Frusemide, ( In the thick ascending limb of the loop of Henle) is the single most important event, that changed the way we manage cardiac failure in both acute and chronic settings. Still, the current evidence creators hesitate to call it a life-saving drug,
The meteoric rise of SGLT-2 Inhibitors
Meanwhile, a few micrometers down the hairpin bend of Henle, drugs called phlorizin are doing wonders. These Apple root barks derivatives were since been invaded by Glyflozins Industry. They are made into a powerful glycosuric drug that drags water out of the system along with glucose. This seems to be the biggest revolution in cardiac pharmacology ever since DaVinci drew the heart and Harvey made it functional. I think we need a supercomputer to count the number of papers and analyze the data from Dapa & Empaglyflosin. It is now concluded officially, as an evidence-based life saver in HF.
I asked one Gen X Pharma-geek, “How do these magic drugs perform this miracle in heart failure”? He said beamingly, It is not merely Glyco-diuresis, as you academicians think, it is some mystery action from heaven, still not decoded. What a revelation I thought.
Continuing Medical Education: Choosing the correct path is never easy!
Final message
Loop diuretics are powerful drugs that aid the failing heart to reduce both pre and after-load. It is a fact, indiscriminate use of these drugs leads to some electrolytes and metabolic issues. But, hiding behind a hazy and shaky evidence base, and trying to ridicule these life-sustaining drugs, is the height of senselessness in cardiac failure literature.
Reference
(There is a tug of war of evidence between benefits and risks. I guess someone will bring out the truth, which is written clearly on the walls)
It is to be noted,Eplerenone (EPHESUS trial ) & Finerinone (FIDELIO-DKD trial) are new generation K + sparing diuretics and mineralocorticoid antagonists may have better cardioprotection in cardiac failure.(Part of RAAS blockade)
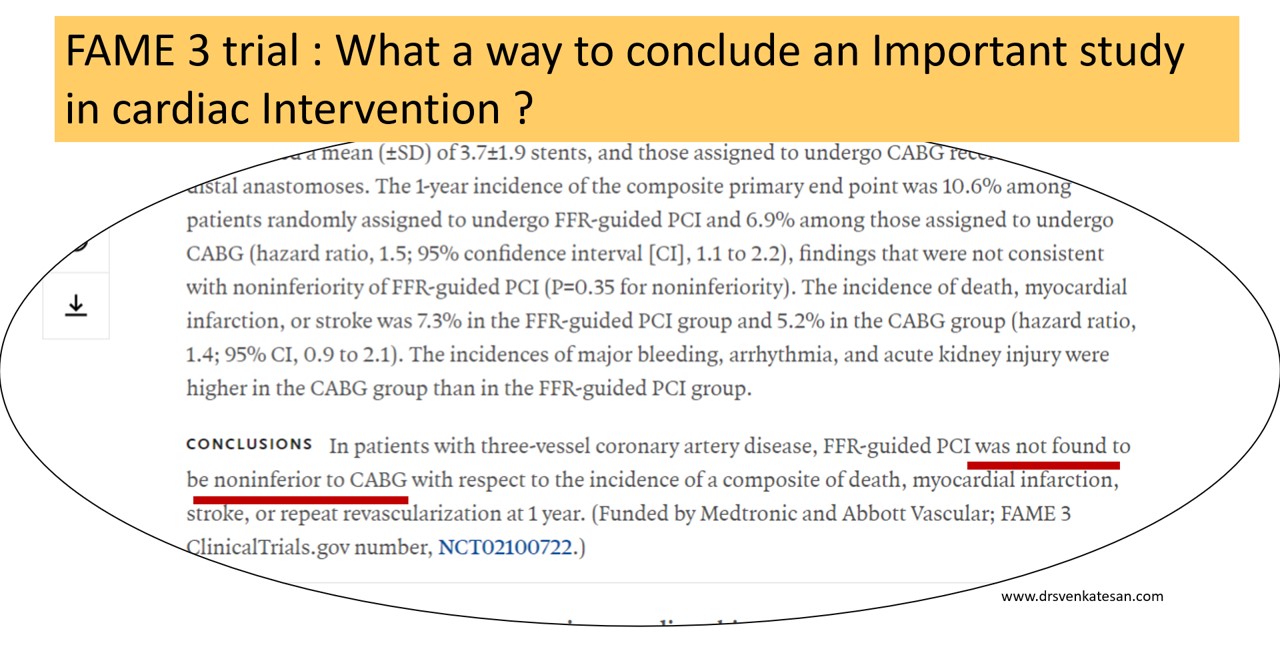
News: Series of clinical trials fail to clear the ongoing confusion in the business of cardiac revascularization.FAME 3 is the new addition.
Caution: A non-academic journal review
There is no secret, about this cold war happening in an incognito mode for territorial rights between cardiologists and cardiac surgeons in glamorous cardiac suits for the past two decades. Of course, we keep believing this is a friendly fight in the overall interest of CAD patients. The ultimate winner should be the patient, not anyone else. Will that happen? Will anyone will allow that to happen? I am not sure.
The FAME3 is a stunning large study from 50 centers FFR guided multivessel PCI, that failed to dethrone CABG (or at least it wanted to sit along with it) I am not a seasoned statistician but definitely can’t understand the logic behind the methodology* and the choice of words in the conclusion from a paper published from a renowned journal.
(*I can recall an article about Non-inferiority trial from Lancet (Ref 1) )
FAME 3 aftermaths: A dizzy Interpretation
Before accepting the fact that, FFR guided PCI wasn’t able to show its superiority or to unable to prove its non-Inferiority, while CABG was clearly found to be non-inferior, (rather superior) to PCI, we should take into account an important caveat in the concept of FFR itself, which has at least half a dozen serious hyperemic and non-hyperemic flaws that demanded a more superior,non-hyperemic indices like iFR, RFR, qFR, etc.
Those of you who still believe PCI would be an undisputed modality in multivessel CAD should take up the challenge and disprove the superiority of CABG by doing the same FAME 3 subset with iFR and other stuff. (Eagerly waiting for the hypothetical iFAME 4 trial)
One more way to Interpret FAME 3: How can we accept FFR guided multivessel PCI as inferior, unless we have an FFR guided CABG (FAME 3 didn’t do this) to compare? Can you guess if only pre-CABG FFR was mandatory criteria, that would have excluded or included important grafts, what would have been the impact of CABG? This is a more dramatic suggestion, that will say sorry to FFR,( the old physiological friend,) and label it as a new villain.
Final message
Multivessel PCI still has a long way to go before trying to dethrone CABG. But, strictly scientific cardiologists need not worry much and they can continue to indulge multivessel PCI without FFR, which is no longer unscientific ! Thanks to FAME 3. I think one of the Important indirect consequences (?purpose) of FAME 3 would be, playing the end game for FFR.
As I understand, we don’t have any. Maybe, we can try this. No way, I can prevent it from appearing ridiculous for the mainstream scientists.
Truths often lie silently buried deep (many times intentionally). They definitely deserve an intellectual resuscitation beyond the dirty world of data and evidence. Further, why should experience be considered as enemy of evidence ?
There are about 30000 scientific journals and two million papers every year. Of which 5000 are in medicine (Ref : World university news)
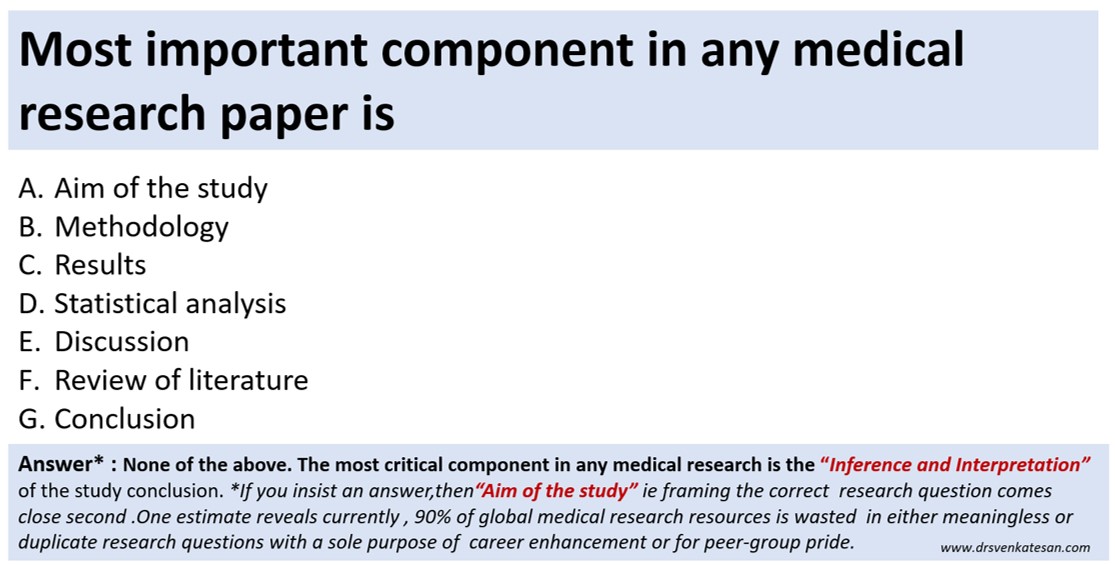
Now, take a deep breath and answer this query. What do you think is the most important aspect of any scientific or medical research in the current era ?
Final message
With due respect to all researchers, What do you think is the most important aspect of any scientific or medical research? This query is very much relevant today. All components are equally important is an easy way out. But, that’s not the pathway that will take us to the truth.
Postamble
Having answered the above question, no way, we can escape from this question –“Which could be the least important component “?
I guess you got it right. In the current scenario, my choice is striking and is sandwiched in the middle of the 7 responses..
“What to do next?. Is he symptomatic? Yes. Definitely has significant angina” but LV function is normal.
“Ok then. If you are daring enough, ask this question”.
Which lesion is causing angina?
No easy answer at all. Try looking for some clues right from history, ECG, stress ECHO, meticulous assessment of individual lesions. Realize, even sophisticated imaging like SPECT, PET functional MR, may not help much either.
Oftentimes, we need to use the lean resources of collective common sense and clinical acumen.
If it is post ACS status, consider residual ischemia in the culprit artery is the cause for angina.
Second, consider the tightest lesion as angina-related.
Or the complex, eccentric, thrombotic lesion is responsible.
Next, consider LAD as default lesion as angina related artery (Statistically right 75%, prognostically perfect decision)
Watch for ECG changes during chest pain (ST depression usually don’t localize, but experience tell us V5 /V6 ST depression is more likely to be LAD ischemia )
Echo wall motion defect either during rest or (more usefully) in stress can really help. (It needs some effort to look for Wall motion mapping with coronary lesion subtending segment)
What about balloon inflation test during PTCA ? . Prompt angina when a lesion is occluded may give a direct clue.
Want to get more confused?
Ask your colleagues for an opinion either online or offline.
Do FFR/QFR/IFR and OCT and look for intracoronary pressure-flow data and plaque burden. We are entitled to get excited about fibrous cap thickness, and hunt for vulnerable lesions and decide thereupon.
Finally some easy options.
Which lesion is causing angina? Never entertain that troubling question at all. (Need not squeeze your coronary intellect you know )
Consider every lesion as important
Get ready to stent all three or more lesions.(Many times forbidden though !)
(or) More convenient, refer to CABG. (Surgeons will welcome for sure )
Final message
Which lesion is causing angina? is indeed an important query one should raise. This paves way for selective focussed PCI in deserving lesions alone. However, when dealing with complex lesions subsets. the most pragmatic way as of today is to educate the patient and include them in the decision-making process (Never forget to offer medical management as a permanent option, especially if there is no critical LAD disease, and say thanks to ISCHEMIA/COURAGE/ BARI 2D.)
Evidence-based medicine (EBM) is being projected as a scientific God’s secret specialty. Physicians who don’t follow EBM are considered unfit non-professionals. Presumably, in pursuit of truth, all those glamorous official bodies in cardiology bring out umpteen number of protocols, guidelines, advisories, and recommendations.
The blueprint for EBM
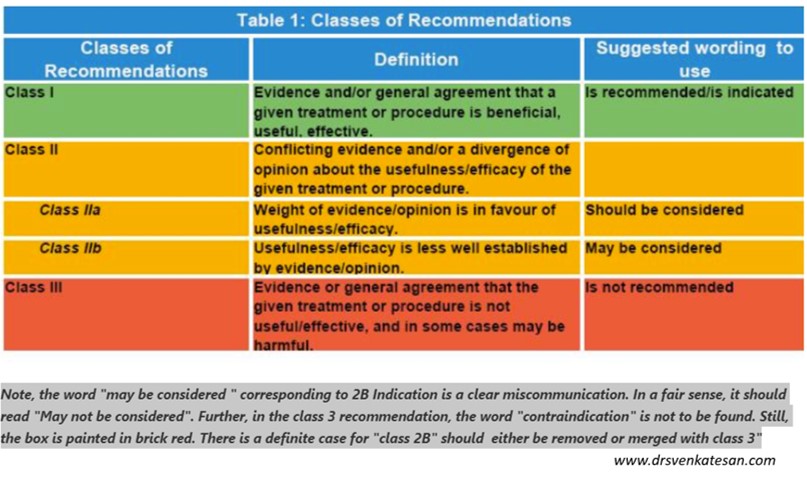
We have the famous 3 levels of recommendation backed up by different levels of evidence. Many of us trust these as the jury’s final verdict for most illnesses in cardiology. I would like to bring one particular issue about this hugely popular model of EBM. It is about one specific class of Indication referred to as 2b. The other day, there was an intense argument for an ICD in a young HCM patient and CRT in DCM based on this 2b stuff. Kindly request all of you to pause for a moment and introspect. We can realize, class 2b plays a mischievous game in EBM with the English language “may and may not”. It tries to push subconsciously an interventional bias from equipoise, in spite of lack of good evidence and clear divergence of opinion and a possible trend towards harm.
Further, there is widespread reluctance in many cardiac workgroups to refer class 3 recommendations as an absolute (or at least relative contraindication) It was strange to note one of my colleagues argued that, class 3 is also a fair recommendation, to accept or reject is in our domain. I was initially shocked to hear that but had to agree with him ultimately as we realized a significant chunk of interventions we do, like delayed PCI > 24 hrs, CTOs, and chronic stable belongs to the proud class 3 recommendation. The debate came to a funny end when a senior cardiologist confessed somehow class 3 seemed to be a lesser evil than even class 2B.
Final message
For the sake of our patients, we need to bring an urgent reform in the EBM. Let us merge class 2b with class 3 and put it in a single basket and keep it out of reach to all tempting stakeholders.We shall display only class 1 in our therapeutic showcase.
Counterpoint
(*Dynamic recommendations is the norm in science, as we accumulate evidence with time.. Agreed, let us do this silently in research labs. Don’t bring it to practical guidelines. No, can’t agree. Freedom to indulge with an experimental modality in a no-option patient must always be there as we are able to give the benefit of doubt to these helpless patients. This is a valid argument but we must not forget even in dire situations good option need not be a compulsive action, it can be in action as well)
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.