Dual LAD is an interesting coronary artery anomaly proposed originaly by Spindola in 1983 .He classified it into 4 types. In recent years the dual LAD has increased from 4 to 6 types.
The essential criteria to diagnose could be summarised.
- Two LADs should be identified.
- One would be large and another small
- Both should give a diagonal branch .
* Ramus is virtually unknown if there is dual LAD .
The origin of second LAD can be from
- LMCA
- RCA
- Direct from Right coronary sinus
Course
- Can be epicardial
- Intra -myocardial
- Or both
Branches
- Diagonal
- Septal
- or Both
Drainage area
- Highly variable
Implication for intervention
- Apart from the surprise element , the second LAD has little impact on the interventional protocol.
- However , it may confer a ischemic protection as the critical anterior wall has a twin blood supply.
- Whether they are protected from primary VT or VF is to be studied because of better electrical stability
- Second LAD may act as an additional collateral channel.
Spindola’s classification of Dual LAD (Types 1 to 4 was called sometimes A,B,C,D )

Source : Lee et al. BMC Cardiovascular Disorders 2012, 12 :101
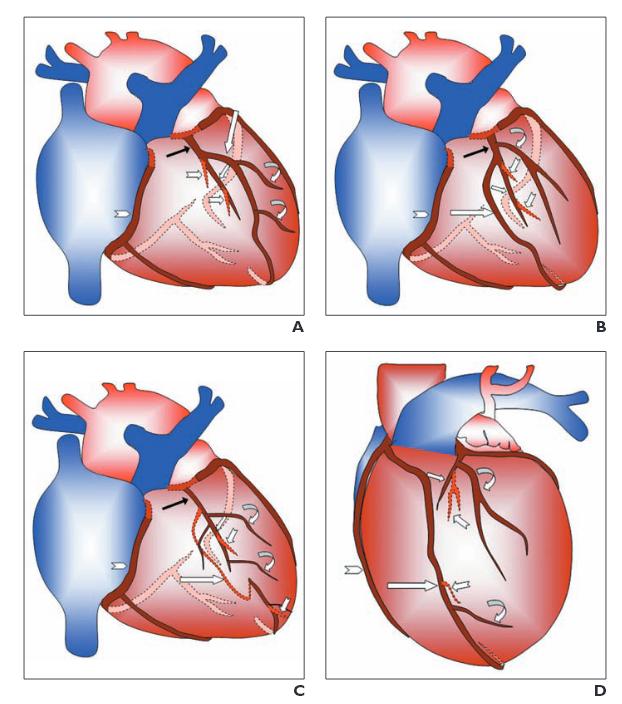
An illustration of first 4 types of Dual LAD .Note the type 4 originates from RCA. Image courtesy : Prachi P. Agarwal Ella A. Kazeroon . AJR:191, December 2008
Surgical issues ( This is excellent data from India . I convey my greetings to one the authors Dr D.B Baruah, my friend from CMC Vellore !)

Reference
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3509398/pdf/1471-2261-12-101.pdf
Dual LAD CT Angiogram : http://www.ajronline.org/doi/pdf/10.2214/AJR.08.1193