As we practice this Noble (& Delicate ) profession ,we often tend to Ignore the warnings even from our learnt colleagues , Why ?
Posted in bio ethics, cardiology innovation, Cardiology quotes, cardiology-ethics, Venkat quotes, Wintage cardiology, tagged aga asd device ado 1 2 figulla flex 2, asd vasd pda device closure, cath lab nightmares, cath lab tricks and techniques, dr s venkatesan, ego vs wisdom, venkat quotes, wisdom quotes, wisdom vs knowledge on July 28, 2014| Leave a Comment »
As we practice this Noble (& Delicate ) profession ,we often tend to Ignore the warnings even from our learnt colleagues , Why ?
Posted in cardiac surgery, cardiology -Therapeutics, cardiology congenital heart disese, cardiology innovation, Cardiology Innovations, pulmonary hypertension, tagged a new avatar for potts shunt, percutaneous potts surgery for severe pah, Potts shunt for eisenmenger on February 18, 2014| Leave a Comment »
Many decades ago Potts shunt (Central Aortic -PA shunt)was used to increase pulmonary blood flow for severe RVOT obstruction mostly for TOF and tricuspid atresia .With the advent of ICR and Fontan role for central aorti shunts waned.
Now, read this
Chronic ,refractory pulmonary hypertension of any cause has dismal outcome.In patients with severe PAH many patients reach supra-systemic pressures . RV a volume handling chamber faces a uphill task of overcoming huge RV after load. As cardiac physicians , we struggle to perfuse the lungs in such situations.
The only option seems to be lung transplantation !
How to perfuse the lungs if the RV is failing ?
Is there any other alternative ?
Why not,use LV contractility to perfuse lungs .
Great Idea isn’t ? After all , how can we allow left ventricle known for it’s robust bumping function sit idle and relax when it’s counterpart is struggling with heavy load ?
How to use LV for increasing pulmonary blood flow ?
Create a central Aortic -Pulmonary shunt.
That’s resurgence of Potts shunt.
Dr Julie Blanc from France suggested this approach in in NEJM as a letter (Potts Shunt in Patients with Pulmonary Hypertension N Engl J Med 2004; 350:623) . It was a great Idea.
Since then lots of patients have a benefited from this vintage surgery.

Final message
A surgery blamed for early onset of pulmonary vascular damage due to potential Eisenmenger reaction is back .Indication for refractory Eisenmenger syndrome to perfuse lungs at very high pressure Nothing is obsolete in medical science .Nothing is ironical as well !
Another Innovation : Now Transcatheter Potts Surgery
Posted in Cardiology - Electrophysiology -Pacemaker, Cardiology -Emerging technology, cardiology innovation, Cardiology Innovations, cardiology journal club, Cardiology-Land mark studies, Future cardiology gadgets, tagged changing batteries in vvi pacemaker, future of permanent pacemaker, implntable rv vvi pacemaker, st jude naostim wirelss pacemaker, wireless pacemaker on October 18, 2013| Leave a Comment »
Few Innovations are real breakthroughs in cardiology . Here is an imminent technology waiting to explode in the permanent pacing . Expected to hit market next year (2014 in Europe ) FDA approves clinical studies .

Click over for the animation video of the procedure .
Future directions in Permanent pacing.
The only threat for this technology is the concept of biological pacemaker Converting ordinary myocytes into pacing cells by genetic engineering.This is expected to happen within few decades.

Posted in cardiology innovation, cardiology journal club, Cardiology journal links, cardiology journals, Cardiology teaching websites, Cardiology-Land mark studies, Great websites in cardiology, tagged great learning websites, INTECH open science open mind, OPEN ACCESS JOURNALS, SCIENTIFIC DEMOCRACY on June 28, 2013| Leave a Comment »
I stumbled upon this web site . I think this can be glorified as the standing example for “Democracy of science”

http://www.intechopen.com/subjects/cardiology-and-cardiovascular-medicine
Posted in Cardiology -guidelines, Cardiology -Interventional -PCI, cardiology -Therapeutics, cardiology innovation, tagged banking and cardiac care, cost of ptca, financial issues in cad, funding for cardiac care, insurance ethics in medical care, insurance in cad, ptca by credit, state vs central government spending for cardiology on May 31, 2013| Leave a Comment »
Heart disease was once considered as rich man’s disease . . . It’s no longer true . We in India , are witnessing an epidemic of CAD . The reasons are varied . Apart from conventional factors , social factors like changing demographic pattern , life style , ethnic risk like south Asian metabolic profile are responsible .
While Rheumatic heart disease (RHD ) continues to be a huge burden , CAD is the number one cause for cardiovascular morbidity and mortality .
CAD affect the poor and rich with equal vengeance . The later is better equipped financially to tackle it . Of course , it has resulted in maximum inappropriate interventions. The poor (or borderline poor ) have no other option but to knock the doors of Government hospitals. It is heartening to note, various state Governments are gradually involving insurance schemes.
Still , many struggle to find the required finance for a major cardiac intervention. It roughly costs 100,000 rupees for PTCA .While PCI is required in all symptomatic , critical coronary occlusions , still . . . majority of the CAD in general population do not require it . There are 675 cath labs in India performing 180000 angioplasties every year on an average of 15000 PCI per month ( 500 /day ) This is grossly inadequate . We have huge potential
What is the hurdle ?
No . . . it is all about financial resources
Recently I stumbled upon an advertisement on Times of India

Disclaimer: This article does not in any way defame any hospital that offers the scheme.It just want to debate the concept.
Hospitals want to market the procedure . Convert angiograms to angioplasties . That’s corporate boardroom mantra . And one fine day , bankers and medical doctor sat together and brought a brilliant idea.
Why not do the procedure on credit and push the patient life long into a financial debt !
Wonderful idea . . . many thought .Thus came the financing scheme for cardiac procedures.
Final message
Financing a poor patient with good intention is welcome. But, there is big caveat .In a vast country with high illiteracy , inappropriate procedures may be thrusted upon on the poor souls.
After thought
Now , our patients have one more risk parameter to assess ” Number of remaining EMI( Equal monthly instalment ) and incidence of stent thrombosis” “Accumulated interest and angina” What a wonderful way to provide cardiac care !
I can recall a patient who sold his livestock (his sole income source ) for undergoing a open heart surgery and lost his life as well in the process leaving the family stranded !
Solution
The only solution is to provide a strictly regulated Govt sponsored insurance scheme. High tech procedures should be continuously and meticulously audited for cost effectiveness .
Posted in Cardiology -Interventional -PCI, cardiology innovation, tagged balloon support and coronary stenting, crossing a lesion with balloon, doubel balloon catheter, gemini stent balloon accuramed, gurentzig innovations in ptca, innovatons in ptca, non compliant balloon in ptca on January 15, 2013| Leave a Comment »
In this complex world , simple innovations fail . . . just because they are simple !
Here is a new* PTCA catheter which has a two balloons , the distal one dilates the lesion and the proximal one has a stent over it . The stent is just deployed after the dilatation by the proximal balloon . The proximal balloon not only help us prepare the lesion before stenting it also helps in crossing difficult lesions . Further , it can be even used to post dilate the lesion . It can be a non compliant balloon as well . It appears a good concept .
*Not really new I believe , Accuramed owns the patent for this twin balloon catheter over a decade now .(First twin balloon Gemini PTCA was used in 1988 )

I do not know why we haven’t adopted it yet , while many dubious innovations are making merry around the world !
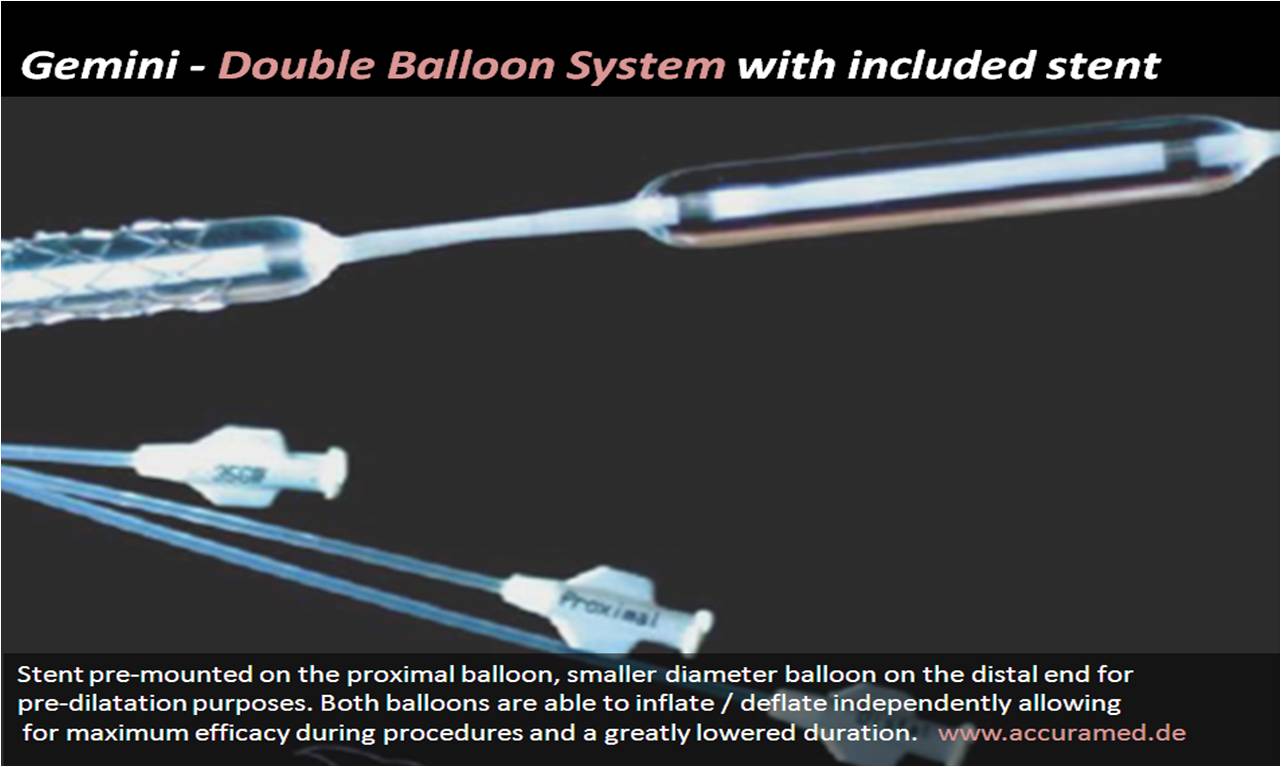
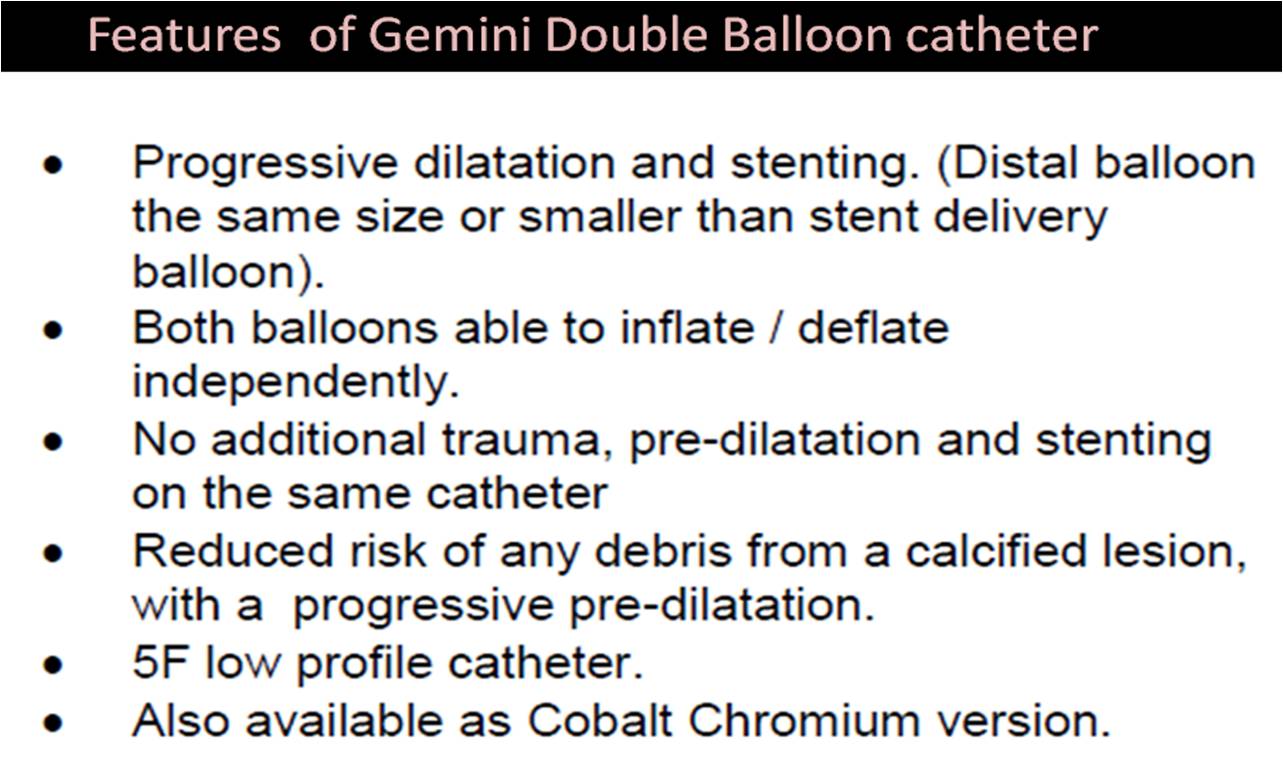
The only downside could be , combinations of stent and balloon sizes are limited . But , it is not a major issue .The ability to fine tune the stent apposition moments after the procedure , by h a simple pull back is just amazing !
This catheter is made by
A C C U R A
Medizintechnik GmbH
Max-Planck-Str. 33 61184 Karben Germany
Tel +49-6039-9201-0 Fax +49-6039-9201-22
E-Mail info@accura.info
http://www.accuramed.de
Final message
Two balloons over a single catheter is a new development .I wonder it can be the standard of care in all PCIs . Hope somebody takes this concept to the next level for the benefit of our patients.
Link to the manufacture
http://www.accuramed.de/fileadmin/daten/en/Gemini_System.pdf
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, cardiology innovation, Cardiology-Coronary artery disese, Infrequently asked questions in cardiology (iFAQs), tagged can we do excercise stress test following primary pci, pre discharge est after primary pci, pre discharge tmt on August 20, 2012| Leave a Comment »
An awkward argument for routine EST following primary PCI
Please remember, primary PCI is not the end of the management of STEMI. Primary PCI is an IRA focused intervention. We need to study other lesions and their the flow pattern as well. Logically we need to do a test for adequacy of baseline vascularity and the current revascularisation . Simple deployment of a stent in IRA (without documentation of good flow during exertion ) is not acceptable to believers of scientific medicine . Resting TIMI 3 flow conveys no meaning for a patient who is going to be ambulant and active. A stress test will come in handy .
The micro-vascular integrity and resistance following an extensive STEMI is best studied by the adequacy of exercise induced coronary hyperemia (This is physiologically equivalent to the much fancied FFR in cath lab ) . One can consider EST following a primary PCI as an non invasive substitute for the collective FFR of all three vessels including the IRA that is stented .
Does any cardiologist have guts to do a pre- discharge EST after a successful primary PCI ?
Typical responses would be
If you think , it is too risky to exert a successfully revascularised patient early after a STEMI . . . at the same time argue to do it in non revascularised patient routinely . Do we not see a huge irony here ?
Other inference could be . . . we are still suspecting the quality of our revascularisation during PCI !
If EST is contraindicated after a primary PCI , are we going to advice these patients against indulging in any activity requiring moderate exertion fearing a stent occlusion ?
. . . What a way to interpret the aftermath of a ‘state of the art ‘ procedure called primary PCI !
In science , correctness is more important than politeness !
Posted in Cardiology - Clinical, cardiology -Therapeutics, Cardiology hypertension, cardiology innovation, echocardiography, Hemodynamics, tagged atrial alternans, doppler echocardiography, e and a velocity swings, mitral inflow alternans, newer concpets in diastolic dysfunction, non respiratory swings in mitral e velocity, pulsus alternans, recent advances in diastolic dysfunction on September 28, 2011| 1 Comment »
Heart is a dynamic organ . It can alter its force of contraction with every beat according to the needs.Generally it responds to length of previous diastole.This is famously called frank starling law , ie the force of contraction is directly proportional to the end diastolic fiber length. So changing diastolic duration as in atria fibrillation classically result in varying amplitude of LV contraction and pulse volume.
However , the commonest cause for pulsus alternans is due to severe left ventricular systolic dysfunction .There has always been a suspicion about the existance of beat to beat variation in diastolic function as well. We have recently observed a new* explanation for pulsus alternans .We know AV inflow is subjected to respiratory swings . Non respiratory swings in mitral and tricuspid valves are rarely described. This pattern is now increasingly recognised.
These non respiratory swings in the mitral inflow doppler pattern is seen in some of the patients with hypertension and LVH.This probably confirms the existence of beat to beat variability of diastolic function . This phenomenon is relatively a new observation . Such pattern are common in patients who have had a recent hypertensive failure .
Here is a doppler of mitral inflow recorded from a patient with hypertension with LVH .

This is the doppler mitral inflow profile of a patient with Hypertension, LVH and class 2 dyspnea .Note the non respiratory swings in both "e" and "a" velocity
It is proposed to define a new class of diastolic dysfunction that can be referred to as diastolic mitral inflow alternans .This phenomenon probably indicates a more severe grade of diastolic dysfunction.At the molecular level this is related to undulating flux in the calcium uptake from cytoplasm into SERCA .There is one more possible explanation for diastolic alternans -Left atrial dysfunction .
Occasionally one can visualise a chaotic pattern of diastolic filling waves (e=a e>a a> e ) Such patterns are thought to be markers of impending acute diastolic shutdown .
Further analysis of this mitral doppler inflow pattern will be reported later.
Reference
* Though we observed this for the first time , this is not a new phenomenon .There are few reports available in the literature.

http://www.sciencedirect.com/science/article/pii/S0735109785800358
http://www.sciencedirect.com/science/article/pii/S0894731706012818
Posted in cardiac physiology, cardiology innovation, echocardiography, tagged dobutamine, dynamic echocardiography, exercise stress testing, hemodynamics of squatting, poor mans stress echo, squat echocardiography, squatting and afterload, stress echo, stress echocardiography, tmt on August 4, 2011| 1 Comment »
There are innumerable stresses to human beings in daily life .
Heart experiences a few either directly or indirectly.
Squatting is rarely realised as a form of physical stress to heart . Rather , squatting can also be termed as a good exercise ( Western toilets sans it !)
Squatting raises the afterload at the level of aorta due to increments in SVR (exact mechanism not clear ,neural reflex ?) and temporary reduction in venous return.
After load raise is synonymous with increased ventricular wall stress . So, it is logical to expect wall motion defect in vulnerable hearts* when confronted with sudden increase in afterload .(*Ischemic hearts with delicate coronary blood flow ) .Hence , sudden squatting , a seemingly simple maneuver , can unmask silent CAD .It can be aptly be named as poor man’s stress echo.
Of course , it doesn’t mean in any way , it should not be used in rich ! The purpose of science is to make things simpler and cheaper . If squatting can replace dobutamine with fair degree of accuracy atleast in a few , it can help control the escalating costs of cardiology triaging due to many futile diagnostics !

http://content.onlinejacc.org/cgi/reprint/46/5/931.pdf
When squatting is a stress in normal persons , paradoxically it gives relief to patients with cyanotic heart disease
Read the related articles in this site .
Posted in Cardiology - Clinical, cardiology -Therapeutics, cardiology innovation, cardiology-ethics, history of cardiology, tagged art of medicine, cardiology update, cme, continuing medical education, discontinuing medical education, hippocrates medicine, history of medicine, jama, medical backdate, medical ethics, medical update, nejm, revisited on May 16, 2011| Leave a Comment »
One of the greatest medical sermon of our times is “Doctors must constantly update their knowledge , Continuing medical education is as sacred as their profession ! If you are not updating your knowledge you cease to a doctor “
It is fashionable , but true to state modern medicine lacks humane care . Modern medicine is challenged by a huge technological , commercial onslaught where common sense takes the back seat
Hence , doctors need to renew not only their academic competence but also their ethical fitness every year !

Aggression could be the other name for modern medical care . For every new invention , treatment or guideline that is approved an equal number is shelved after few months or years for safety reasons.
Bulk of medical updates for current age physicians is nothing , but asking them to forget all those wrong things that has been meticulously uploaded in their brains in the recent past ( Recall the classical story of drug eluting stents )
If this is the case . . . then . . . what for we are updating ? and for what we are learning and forgetting ? and . . . how frequent we need to forget ? Of course , there is a big chunk of human tribe who can never master the art of forgetting ! Some mistakes are permanently etched in their terra byte hard disks .
Is there a place for backdating and discontinuing medical education ?
What man- kind needs at times of medical crisis , is not the current treatment but the correct treatment .It is our duty to find all those trustworthy drugs & treatment modalities that were sent to the gallows by the modern medical forces for various reasons !
If some of the gems in medicine are left behind in past “time domain” , it is mandatory for us to go back in time and catch it , adopt it and disseminate it !
Further , whenever the hyped “medical updating sessions ” turns out to be synonymous with adding nonsense (It is becoming all too common these days !) we should resist it by all means !

For many . . . Hippocrates and his medicine sounds dirty now !
If only we back-date our knowledge . . .
Todays youngsters can learn a secret that liver enlargement can be diagnosed easily with their hands , without waiting for a CT scan report !
If only we back-date our knowledge . . .
We can realise Aminophylline can save so many lives of cardiac failure , which our newer inotropic agents are struggling to accomplish .
If only we back- date our knowledge . . .
We can calmly manage acute MI with lignocaine even in a country side . Amiodarone unfairly replaced this efficient anti VT molecule for no academic reasons !
If only we back- date our knowledge . . .
We can advice simple non pharmacological intervention for stage 1 HT than prescribing the glamorous sartan molecules form a multinational ARB shoppe.
If only we back- date our knowledge . . .
We can promptly recognise cardiac failure without ordering for the error prone BNP . Back dating also helps us to under stand that post infarct angina is a glaring sign for presence of viable myocardium and prevent us from undertaking a 2000 $ PET excursion !
If only we back- date our knowledge . . .
We can send all our uncomplicated , asymptomatic STEMI patients ( in class 1 ) straight to their home rather than to cath lab play grounds !



