An Interaction in IMCU
How is Mr. K, who was shifted from ward 102 ?
Yes sir, It was acute decompensated LV failure, Patient was in impending pulmonary edema. In fact, he developed. He is fine now,
How did he come around? He was too sick I thought.
“Just pushed 60 mg Frusemide IV, luckily he also had good BP, so with an infusion of NTG, titrated Carvedilol a little bit, he came out nicely. I guess it is Ischemic DCM”.
“Good, You have done a nice job”
“Don’t make me embarrassed sir. It is such a routine in our ER.
To make him curious, I asked “Which drug do you think that saved him”?
“Obviously, Frusemide sir. He was frothing out. I thought he will require a ventilator. It was a matter of 20 minutes, sort of flushing out 500 ml lung fluid through the urine”.
“No, you are wrong. As a professor and cardiologist, I need to tell you this. Diuretics never save lives heart failure.
Sir, I guess, you are not kidding. Does this statement apply to acute heart failure? We have saved 100s of lives with Frusemide, both in acute, acute on chronic, and even in chronic cardiac failures with metolazone.
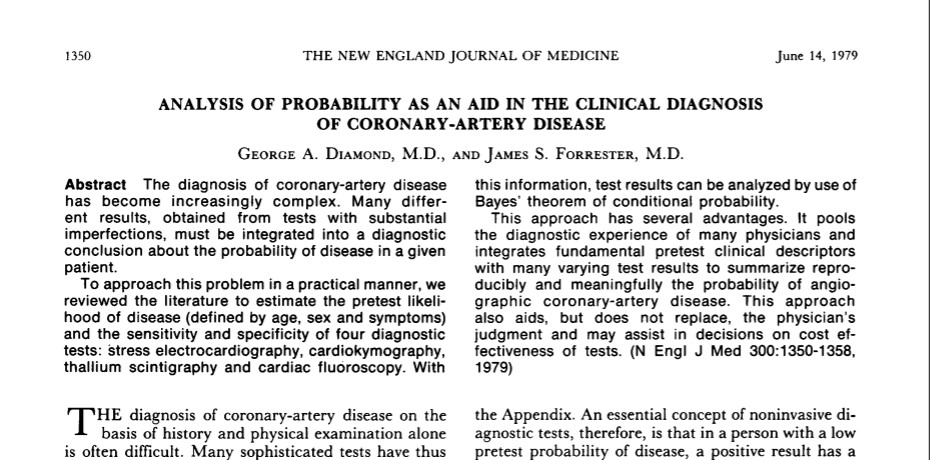
Hmmm, I agree with you my dear student, Frusemide has saved not hundreds but lakhs of lives in the past decades in all forms of heart failure. It continues to do this fabulous job even now. But, don’t say it in exams or scientific forums. It has no evidence to show survival benefits. You can’t credit a drug without evidence. Also realize, saving lives by unscientific means by a cheap generic is not something to boast upon. We need the blessings of RCTs, or Kaplans Mayer curves, or Forrest blobbograms. Unfortunately . that is the current principle of practice of medicine.
But sir, who is preventing whom, to do such studies. Why they are not comparing diuretics one to one with these modern drugs of inotropes, calcium modulators, or SGLTis, etc?
I am not sure. My guess is, there are no good friends in the cardiac failure research community for this old warrior drug.
Loop diuretics
Till 1960s, toxic mercurial compunds was the only option to drain water in heart failures. The Invention of Na+/K+ /Cl channel blocker Frusemide, ( In the thick ascending limb of the loop of Henle) is the single most important event, that changed the way we manage cardiac failure in both acute and chronic settings. Still, the current evidence creators hesitate to call it a life-saving drug,
The meteoric rise of SGLT-2 Inhibitors
Meanwhile, a few micrometers down the hairpin bend of Henle, drugs called phlorizin are doing wonders. These Apple root barks derivatives were since been invaded by Glyflozins Industry. They are made into a powerful glycosuric drug that drags water out of the system along with glucose. This seems to be the biggest revolution in cardiac pharmacology ever since DaVinci drew the heart and Harvey made it functional. I think we need a supercomputer to count the number of papers and analyze the data from Dapa & Empaglyflosin. It is now concluded officially, as an evidence-based life saver in HF.
I asked one Gen X Pharma-geek, “How do these magic drugs perform this miracle in heart failure”? He said beamingly, It is not merely Glyco-diuresis, as you academicians think, it is some mystery action from heaven, still not decoded. What a revelation I thought.
Continuing Medical Education: Choosing the correct path is never easy!
Final message
Loop diuretics are powerful drugs that aid the failing heart to reduce both pre and after-load. It is a fact, indiscriminate use of these drugs leads to some electrolytes and metabolic issues. But, hiding behind a hazy and shaky evidence base, and trying to ridicule these life-sustaining drugs, is the height of senselessness in cardiac failure literature.
Reference
(There is a tug of war of evidence between benefits and risks. I guess someone will bring out the truth, which is written clearly on the walls)
1. Chris J Kapelios, Konstantinos Malliaras, Elisabeth Kaldara, Stella Vakrou, John N Nanas, Loop diuretics for chronic heart failure: a foe in disguise of a friend?, European Heart Journal – Cardiovascular Pharmacotherapy, Volume 4, Issue 1, January 2018, Pages 54–63, https://doi.org/10.1093/ehjcvp/pvx020
Postamble
It is to be noted,Eplerenone (EPHESUS trial ) & Finerinone (FIDELIO-DKD trial) are new generation K + sparing diuretics and mineralocorticoid antagonists may have better cardioprotection in cardiac failure.(Part of RAAS blockade)