

Syncope by definition is a transient loss of consciousness due to cerebral hypo perfusion and loss of muscular tone, and the patient falls but recovers fully and gets up either assisted or spontaneous.The cardiac and vascular counter response to syncope is most often intact .This makes syncope characteristically transient . If a patient does not recover from syncope it could either be a prolonged loss of consciousness( Stroke etc) or if he never gets up he will be called a victim of cardiac arrest or a SCD ! (Sudden cardiac death ) . So technically by defintion , all patients will have to survive the syncopal episode.
But the following questions need to be answered
- How prolonged a syncope can be ?
- Can syncope lead onto sudden cardiac death ?(SCD)
- What are life threatening syncope and non life threatening syncope ?
What is the link between, syncope and SCD in patients with ventricular arrhythmia’s ?
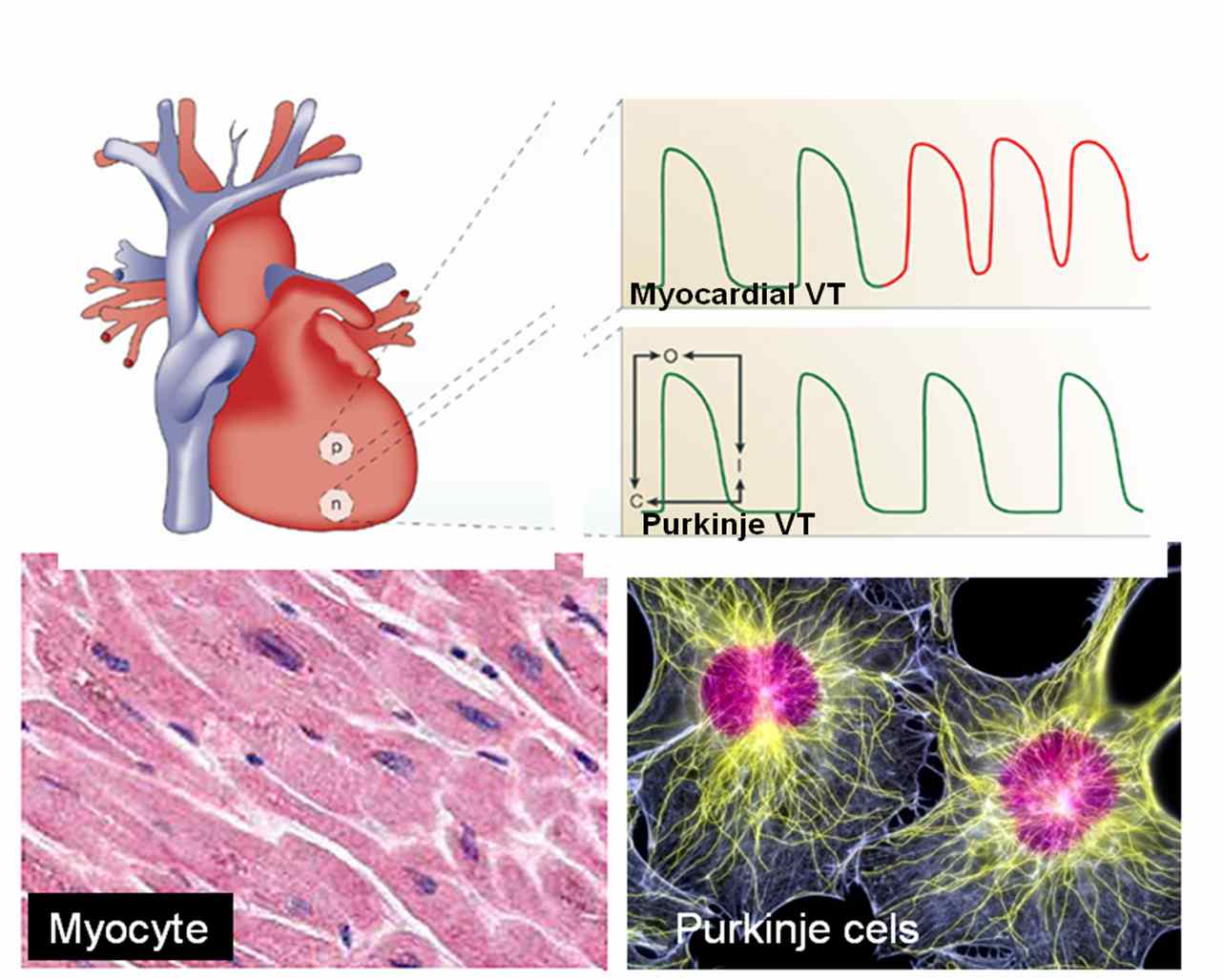
Some case of long QT syndromes could be life threatening especially in children as they inherit sudden death. A patient with a non sustained VT may develop syncope if the VT becomes sustained especially if there is underlying heart disease and LV dysfunction . Among this few , may degenerate into ventricular fibrillation and patient may die.
Prolonged syncope , TIA, stroke in evolution and completed stroke can be a continuous spectrum in patients with carotid and cerebrovascular disese . But when a syncope evolves in to a stroke the patient is not considered to be a victim of syncope but they enter the stroke protocol.
There is a big list for the causes of syncope
But to put it simply
A.Cardiac
- Purely electrical ( Arrhythmic- Brady, Tachycardia)
- Mechanical( Valvular obstruction, and other structural heart disease etc)
B. Non cardiac
- Vasovagal (Commonest 90% of all syncope)
C. Metabolic*
- Anemia
- Hypoglycemia
- Hypoxia
How to work up a patient with syncope ?
First , one need to confirm it is indeed a syncope . If the initial examination is not clearcut one need to go back to the history and ask for circumstances under which the syncope occured and details of prodromal symptoms if any . Patient’s family members who witnessed the event can give useful information . It is the most cost effective ( Comes free of cost infact !) investigative tool available .Cardiac syncopes are usually sudden, vasovagal often have environmental or emotional factor. Apart from routine investigations , ECG, Echocardiography, holter are done generally, head up tilt test, Loop, event recorders may be reuired in few.
Final message
Syncope is one of the common symptoms in cardiology and general medical practice. Many times the diagnosis is easy . Common syncope is never fatal but , ruling out dangerous tachy and bradyarrhythmias is a key aim. In a significant number (20-30%) identifying the cause could be really difficult and may never be made in spite of the modern diagnostic tools. These syncope of unknown origin is grouped along with the neurocardiogenic category.
The one, positive thing about syncope is (unlike chest pain) , it is rarely fatal in it’s first episode , gives the physicians to investigate and correct the underlying problem.
















{kind=link}
{kind=link}