Posts Tagged ‘bmj’
The epicenter of a crisis in modern medical care
Posted in Uncategorized, tagged bmj, british journal of medical ethics, dr venkatesan s, jam network, lancet, madras medical college, medcial ethics, nejm, quotes on medical ethics on June 7, 2026|
Let us go back to the golden age of simple clinical trials & get rid of big, motivated RCTs.
Posted in Uncategorized, tagged bmj, clinical trials, evoultion of clinical research, jam network, lancet, medical education, medical ethics, nejm, rct on April 19, 2026|
Very soon, blogs and independent writing will be the only source of unadulterated truths. One such article is shared here written by Adam Kroetsch , formerly in the FDA
A review and comments
The above article compellingly recounts how clinical trials evolved from ad-hoc, investigator-led efforts in the mid-20th century to the bureaucratic behemoths of today. It highlights the “golden age” of the 1980s-1990s, when academic “trialists” pioneered large simple trials like ISIS and GISSI. These mega-trials enrolled tens of thousands with minimal protocols ,one-page forms, no routine monitoring or source data verification (SDV), proper randomization, and focus on clinical hard endpoints and mortality delivering transformative, low-cost evidence on treatments like streptokinase and Aspirin.
The decline followed the rise of Contract Research Organizations (CROs) in the 1990s, global Good clinical practice -GCP guidelines (1996), and FDA missteps. Trials are now industrialized and bureaucratized: extensive on-site monitoring, exhaustive adverse event reporting, data audits, and risk-averse compliance layers inflated the costs (rising 10% annually). Academic and NIH-funded large trials plummeted .Pharma shifted to smaller, often useless biomarker-driven studies instead of clinical outcome. (Eg Drug X reduce NT-pro BNP by this,and it is crowned in glory ). The irony is ,the trialists are crying “foul” at GCP, and call it unscientific as they interupt the industry.
Who is responsible for this chaos?
Primarily commerce and greed in a profit-driven ecosystem .Alos pharma’s risk aversion and demand for speed and volume. Other factors were, heavily empowered CROs, Perverse incentives and Industry balance sheets, dictated the how science should behave. No surprise , true academics and genuine funders retreated amid prohibitive costs.
Final message
GCP is not a taboo subject, as some non- academic forces would like to envisage. Let us bring back the golden age of simple trials—even observational ones will bring the truth when done appropriately .Let us stop this big commercialised RCT nonsense with ultier motives.
Forbidden quotes in medicine : Healing shall prevail over harming
Posted in Uncategorized, tagged bmj, british journal of medical ethics, dr s venkatesan, ethics in medicine, famous quotes on medical ethics, Hippocratic oath, indian journal of medical ethics, lancet, madras medical college, medical education, modern medicine, nejm, venkatesan sangareddi, world health organisation on April 9, 2026|
Why Superior Scientists, will never rely on Non-Inferiority trials?
Posted in Uncategorized, tagged bmj, data torturing, fake science, fake stastistics, jama network, lancet, medical stastistics, nejm, non inferiority trials, stastistics, who is superior scientists, why rcts are riggged on April 4, 2026|
Statistics is the most advanced form of mathematics by which predictions about the future can be made with some degree of surety. It is a vital cog linking biology with maths. However, since the last few decades, an abnormal man made bio-mathematical mutation is being spotted in the field of medical statistics.
Why superior scientists avoid Non Inferiority (NI)trials?
They avoid relying NI -trials due to fundamental statistical, interpretive, and ethical weaknesses that undermine rigorous evidence and patient benefit.
Superiority trial models , reduce bias towards the null hypothesis and proactively protect against false claims. NI trials just do the opposite. The same issues dilute differences, biasing toward falsely concluding the new treatment is “not unacceptably worse” than the active control by a pre-specified margin . Without a placebo arm, sensitivity cannot be confirmed, and the assumption remains tentative.
Key vulnerabilities In NI trials include arbitrary, manipulable margins that may permit clinically meaningful inferiority. High success rates (>85–95%, especially industry-sponsored) suggesting bias, and risks ( Biocreep) where successive approvals erode standards. “Non-inferior” does not mean equivalent .It can mask statistically significant inferiority. Reporting often deviates from guidelines, with inconsistent margin justification and analyses (ITT vs. per-protocol).
Ethically, NI designs accept potential efficacy loss for unproven gains (convenience, cost, safety) without direct proof, exposing patients unjustifiably in high-stakes areas. They place disproportionate proof burdens on de-escalation or alternatives while entrenching suboptimal standards.
A Lancet Oncology piece highlights this as “the tyranny of non-inferiority trials”:. The authors propose abandoning superiority/NI distinctions for simple “comparative” trials.
Final message
Superior scientists prefer superiority or hybrid designs, or direct comparisons of net patient-centered outcomes .They never go for the NI shortcuts driven by regulatory or commercial pragmatism.
Reference
Many second opinions might be wrong too … consume it with caution !
Posted in Uncategorized, tagged appropriate procedure, bio ethics, bmj, british journalmof medcial ethcis, clinical decision making, dr s venkatesan, esc, inappropriate interventions, lancet, madras medical college, medcial decsion making, medcial errors, medcial ethics, medical education, medical incompetence, nejm, pateint empowerment, principles of practice of medicine, private vs public health, second opinion, third opionion, venkatesan sangareddi, what ails modern medicine on March 8, 2026|
Getting a second opinion from another expert is a valuable option for our patients when they face a complex decision-making process, especially when a cardiac intervention is advised. No doubt, it is their fundamental rights too.But this could be hard, if the second opinion is sought regarding indication for coronary or interventional procedure.
It is much, much comfortable to concur with the original decision if it is pro -Intervention. (even if it is against your conscience). Vetoing a procedure which was advised by some big hospitals is almost impossible for cardiologists sitting at their office, however experienced they may be. This is because it is sort of going against, the mainstream and defying science as well. Both doctors and physicians are stuck.

I confront such situations often from patients following elite cardiology consults. I had been forthright and genuine and said a firm no or yes to many such procedures . I understood much later, that only a minority of the patients followed my No advice , while invariably they accepted my yes.
After much confabulations , recently, I have made some recalibarations on my values, (decent term for compromise ) despite all the ethical stuff I write in these columns. But, three things I ensure , before giving my opinion which goes against my assessment.
“This procedure is not indicated in the true scientific and moral sense, but 1.If you lack full trust, or 2. If you are not ready to accept the risks of not doing it, or 3. If the fear (of not doing it ), would nag you constantly, then get it done as per the advice of the big guys”.
Final message
Until we acquire the courage to express our true opinion , we certainly fall under the tag of medically incompetent.
Very soon, getting a second* or even third opinion may not really matter. Doctors are silently persuaded to follow the guidelines thursted by big scientific syndicates along with compulsion to go with patient wish & preference.
*Caution and clarification
Second clinical opinion for helping to arrive at a medical diagnosis is of immense value and a great thing to do. In fact, doctors themselves ask for it when they are in doubt. This article is about second opinion regarding the appropriateness of various interventional procedures that is defining modern medicine.
How is that ? A self prescribed PCI (s-PCI) , is an accepted professional medical decision
Posted in Uncategorized, tagged acc, aha, bari 2 d, bmj, courage, esc, fear driven pci, ffr, ffr driven pci, guideliens cad, indication 2a vs 2b, indication for pci in cad, insurance driven pci, iscehmia driven pci, jama net work, lancet, nejm, oct, pci, scai, symptom driven pci on March 7, 2026|

Decision making for PCI in chronic CAD continues to be delicate. This is especially true, if the lesion is Intermediate and the plaque vulnerablity is susepcted.
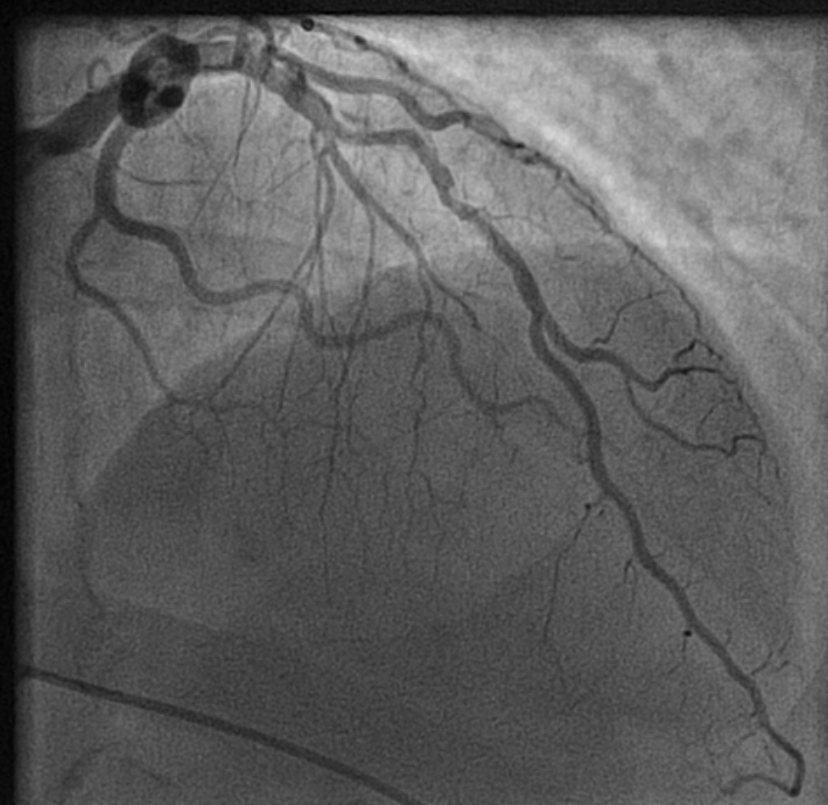
How to tackle this stress positive Intermediate LAD lesion. Functional capacity good. Non-diabetic, mildly elevated lipids. Now, continuing medical management with intensive lipid control is the best possible management. (We have evidence for medical management being good even in significant 90% lesion) Above is a case report from https://www.acc.org/education-and-meetings/patient-case-quizzes/medical-therapy-for-cad
Reassurance is a revascularization equivalent
Sharing a similar experience with one of my patients in his early fifties. After getting a fairly convincing consultation, he accepted medical management. However, guided by both NI & AI, he sought a second opinion to confirm whether my assurance was indeed correct. He underwent FFR and OCT, and both he and his plaque became vulnerable. The FFR was normal. He was too intelligent to ask about the FFR – Stress test discordance, for which his cardiologist had no answer. Still, they did not advise a PCI and the decision was left to him, respecting the current patient-oriented guidelines.
The patient went home empowered but spent sleepless nights, fearing about potential fissures, in the life sustaining fibrous cap.He believed that he was at the mercy of a 75-micron thin cap covering his plaque. In one of the anxious days,in the following week , he got admitted himself in a posh downtown cardiac center. A as per the guidelines, the patient chose his own pathway for a PCI. Cardiologists obliged piously to his wishes. Now, he feels better. He says he is happy to undergo a self prescribed stent.
I was glad, he had the courtesy to come back and showed the results. I learnt. it costed him 6 Lakhs and his insurance covered it fully. I realised , my 30 minutes reassurance was busted by the insurance card in few minutes. I wasn’t surprised.It’s okay, it’s all in the game. I learned it long ago. Fear* (either spontaneous or induced), the power to decide & affordability are the most powerful determinants of any inappropriate medical procedure.
Learning cardiology from UN & WHO
We have United Nations and WHO, the two global guardians. Any one with average intelligence will agree, these instituions can never bring either peace or health to this world.Let us ensure, the practice guidelines of cardiology doesn’t go that way. We boast ourselves, that we have a strongly evidence based vigorously scrutinized cardiology practice framework. How true it is ? Are we hiding behind pateint preference, and pushing science to the background ? Let us be transparent. I think it’s time, the powerful bodies like ACC/ESC should connect all the missing dots. .One important issue is, fear or anxiety-driven PCI, which usually overtakes other true indications.
Final message
In an ideal world , reassurance and GDMT , if properly done, should be a revascularization equivalent in most CAD patients .The reality is, fear* prevails over reassurance, for a variety of reasons.
Postamble
*Anxiety thrives well, in an environment of uncertainty. It is mutually inclusive among both patients and physicians.However most Professional physicians are expected to tackle it. Still many struggle. Patient : What if the block worsens? Physician: What if the patient comes back with an event and oh .. my pride and practice? May be, physicians are not to be blamed much. I think. it is all about a unexplained, biased human mind set. Even a death during an inapproproate Intervention is pardoned off, but an error, raising out of an appropriate medical mangment is rarely forgiven.
Science can wait … not the suffering patients!
Posted in Uncategorized, tagged best medical quotes, bmj, hippocrates, jama dr s venkatesan sangareddi, lancet, medical ethics, nejm, osler willam, pateint care vs science, practical bio ethcis, primum non nocere, science and ethics on January 14, 2026|
AI clinical consults : Beware of machine hallucinations, that could become a permanent medical record of your patients.
Posted in Uncategorized, tagged AI assitted consultation in hospitals, AI consultations, AI in medical profession, ai in medicine, annals of internal medicine, Artificial Intelligence in cardiology, bmj, jama network, journal of AI in medicine, lancet, nejm on December 6, 2025|
It is predicted, (or already happening ) atleast 30 % of clinical consults happen with AI assistsnce or with completely with machines.

The Initial work up is suggested by the AI bots, even in ER rooms. They may be right in 80% of times. But, who is it to filter and grab those remaining 20%. No one , except a astutely learnt clinician. Unfortunately, there is no super AI to do this job.
Final message
This is the beginning of, a new exciting & dangerous era, for the medical profession. If we are not vigilant or loose our common sense, these bots will soon reach their next destination, ie patient’s bed side.
Reference
BMJ in its current Issue address these aspects of increasing AI usage in the clinical consults
1. Clinical competencies for using generative AI in patient care BMJ 2025; 391 doi: https://doi.org/10.1136/bmj-2025-085324
What is the realistic definition for “fact vs fake” news
Posted in Uncategorized, tagged bmj, dr s venkatesan, expressions in cardiology, fake vs fact in medical science, jama network, lancet, madras medical college, medical education, medical ethics, nejm, quotes in medical ethics, venkatesan sangareddi on November 18, 2025|
Trying to become a truly Professional Physician !
Posted in Uncategorized, tagged bmj, ethics in cardiology, ethics in medicine, Hippocratic oath, jama network, lancet, medical ethics quotes, nejm, who is a professional cardiologist on August 10, 2025|
.
Post-amble
Are you a professional physician doctor ?
Honestly I am struggling to become one , it is still a long way to go.
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- July 2026 (3)
- June 2026 (9)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,700,707 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

