PV isolation or ablation is considered as an ingenious modality in tackling chronic recurrent AF. Still, it is too invasive and complication-prone, with less than desired success rates. EPs are struggling to mitigate the adverse events. Hardware has vastly improved. We have since moved from RF , cryo , to pulse field ablations.
Whatever said, AF is a chaotic arrhythmia. When we try to take on the chaos head-on with more force, considerable damage, mostly invisible, is expected in the atrial battlefield. One such thing is post-ablation atrial tachycardia. The exact incidence is under-reported. Many times EPs don’t consider this as a complication at all. It is funny, some percieve it as a partial success as the chaos has become less intense. The fact of the matter is, an AT can be more unpredictable and carry electrical morbidity, whike the risk of further AF always remain.
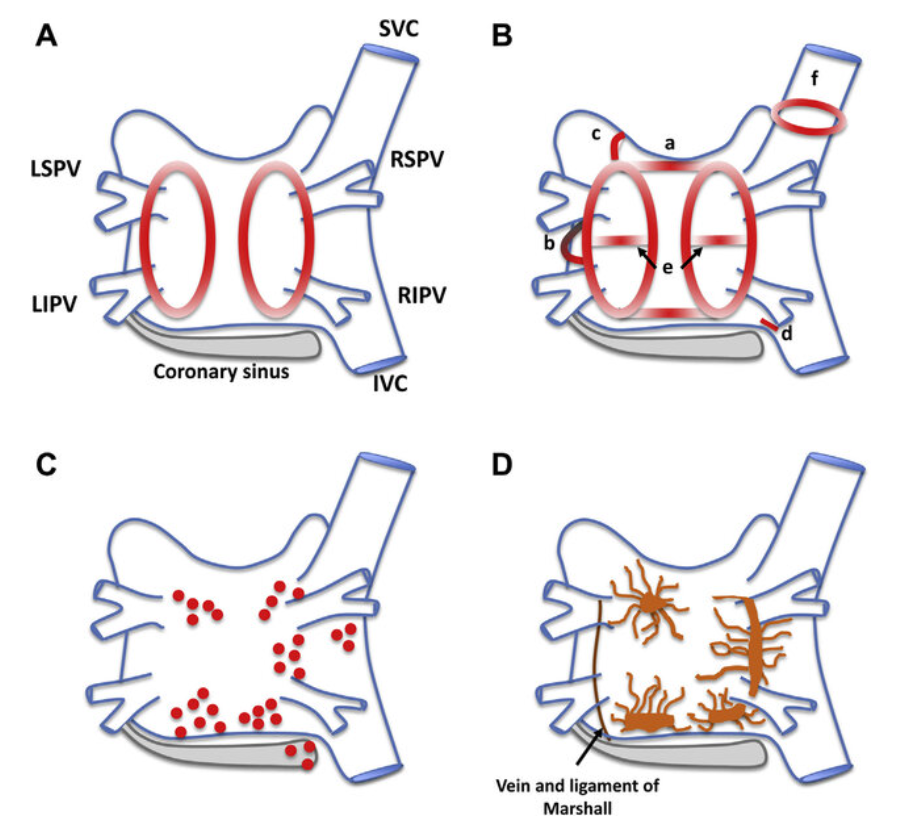
Organized atrial tachycardias (ATs) occur in 5–40% of patients after catheter ablation for atrial fibrillation (AF), with the exact rate depending on the index procedure strategy, AF duration, LA size, and follow-up duration.
With pulmonary vein isolation (PVI) alone: Incidence is lower (5% or less). When AT occurs, it is frequently focal, most often originating from reconnected PVs
With additional substrate modification (linear lesions, complex fractionated atrial electrogram ablation, etc., common in persistent AF): Incidence rises to a prohibitive 20–50%.
Macro-reentrant ATs also occurs due to gap-related peri-mitral or roof-dependent circuits.
Final metssage
Both focal and non focal ATs are much common after PV ablation, than we realise.Very often, they require another procedure or more intensive drugs . Realistically, the original purpose of treating the chronic AF is lost , if AF is likely to be transfomed to some other form of AT.There is nothing called 50% chaos reduction in AF treatment.
The famous & popular 3-24 hr time window for pharmaco-invasive strategy (PIPCI) was adopted, blindly from STREAM (prehospital Tenecteplase + PCI <6-24h in <3h presenters) and FAST-MI trials assuming uniform IRA patency. It fails to stress the importance Initial time window to lysis, and its response . This makes the distinction between true rescue vs routine pharmaco invasive PCI a hazy excercise . Thus, both inappropriately delayed or a hastily-routine PCI has become all too common.
The 24-hour upper cutoff in pharmacoinvasive strategy serves to prevent reocclusion, or to address any residual mechanical stenosis . It is not meant for myocardial salvage, which is irrelevant if lysis was successful.
Mind you, IRA optimisation is not a time bound emergency in a well recannalised vesseel. In fact, PCI is not an absolute neccesity for long term IRA patency especially if it an coronary erosion. If there is TIMI 3 flow ,and there is little ischemic substrate , there is no need to chase the , supposedly sacred 24 hr time window. If the lysis achieves complete( or almost complete) IRA patency, PCI can safely be extended to 48-72 hours, or even permanent deferral (No-PCI , stand alone thrombolysis) in stable patients with optimal medical therapy.
An interesting study is published , from my institute in the current issue of AJC with a title ” Extended Pharmacoinvasive PCI Compared to Primary PCI: Insights From Madras Medical College STEMI Registry” . This study argues for extending the time window for pharmacoinvasive strategy to 48 hrs. (It could still be higher.) It suggests , this flexibility suits the LMIC, due to logistical realities. ( Glad to be listed as a co-athour)
I am sure, this study, demands to reset the 24 hr upper limit of cut off for pharmaco invasive strategy.Looking beyond this study, there is an urgent need to clarify the specifc purpose of the generalised time window of “3 to 24” hr time window in pharmaco invasive strategy.
A call for new sub defintions in the time windows in PIPCI
1.Successful Lysis* (TIMI 2-3, in about 70%): Routine angiography/PCI 3-24h (prevent reocclusion/residual stenosis) .Extendable to 48-72h + is possibel. Permanent deferral if the pateint and myocardiumare , with a patent IRA . (Implying no need for further salvage at all , we should allow a green corridor for patients with successful standalone thromolysis to exit the hospital without a PCI ) Doing a PCI onlu t0 prevent fear of reocclusion in the first 30 days is not backed with good data.
2.Failed Lysis* (TIMI 0-1, 30%): Rescue PCI immediately (<3-6h post-lysi, like PPCI) Here the time window should be hastened and can never afford to extend it, at any stretch of imagination.
* Ironically, the 24hr cut of has no place in both the above subsets. (May be in failed lysis , 24 hr cut off might apply , again it is 12 hr longer than primary PCI )
Final message
“Time is no longer muscle , if the Intial lysis is successful“
What is the purpose of “24-hour” upper limit cut of time in pharmaco invasive strategy ? The 24 hr is not universally valid. Pharmaco Invasive strategy time windows need to be based on timing and efficacy of the Initial lysis.
Postamble
Commenting this paper as a third person :
One limitation in this study is to be admitted. I think, the generalised comparative efficacy of extended PIPCI with primary PCI can not be made, for the simple reason, the extension of time window is possible only in patients who had successful lysis. This study may ideally be concluded as “3-24h pharmacoinvasive PCI can be extended to 48h if the initial lysis successful” . Further, If initial lysis fails (30% TIMI 0-1), any extension is contraindicated and requires immediate rescue PCI akin to PPCI. Also, data regarding non-IRA intervention might help understand the importance of the extension of the time window better.
Ischemic Coronary artery disease is probably the most common medical ailment in humans.
It is managed by four strategies by modern day cardiologists.
A.Only life style modification.
B.Intensive medical management (Also called as GDMT or OMT)
C.PCI
D CABG
Which one of the above modality is considered superior (& popular) among physicians and patients ?
No doubt, PCI is the undisputed winner for all the wrong reasons.
PCI success lies literally at the mercy GDMT. CABG has the same story to tell. While, only GDMT, has the vigor to stand alone in style and triumph in most CAD patients. It needs no great wisdom, to acknowledge, GDMT never gets its due respect. The problem is ,we are all part of those guilty cardiology professionals, who silently watch the PCI, shine in false glory.
A. Very Often. We don’t really require the anatomical Information. A well performed stress test will tell us the presence and significance of obstructive lesions .
B .Majority of CAD patients will require CAG , as we can’t rely on other non invasive tests.
C.Atleast all ACS need CAG, but many CCS don’t need it.
D . Forget about it .It is unethical or rather blasphemy to treat CAD without knowing coronary anatomy.
Pathways to an answer.
Even acute STEMI can be managed without initial ( or even permanent) knowledge of coronary angiogram in atleast 70% of pateints.
* It is sad truth, the modality of standalone thrombolysis has been brutally stigmatised and being portrayed as incomplete and Inferior form of treatment in STEMI. It is pity , such a perception is deep rooted in many cardiologsist’s mind inspite of the fact great studies exists to prove treating STEMI without knowing the anatomy( ie prehospital lysis) could beat PCI consistently )
**How often we need CAG in Chornic CAD? You know the answer . If moderen day cardiac Intervetions insist us take a decision based on Physiology, then why do we want to know anatomy?
A stress test, technically is , equivalent to simultaneous multivessel FFR or iFFR . If some one crosses 10 METs in a stress test , whatever the lesion subset, it can be considered net-equivalent for a normal FFR of near unity. (No one has tested this hypothesis, so as of now it is junk science.) Still every experienced cardiologsist would acknowledge the truth in this.
D. Can never answer this question without X ray or the implantation records.
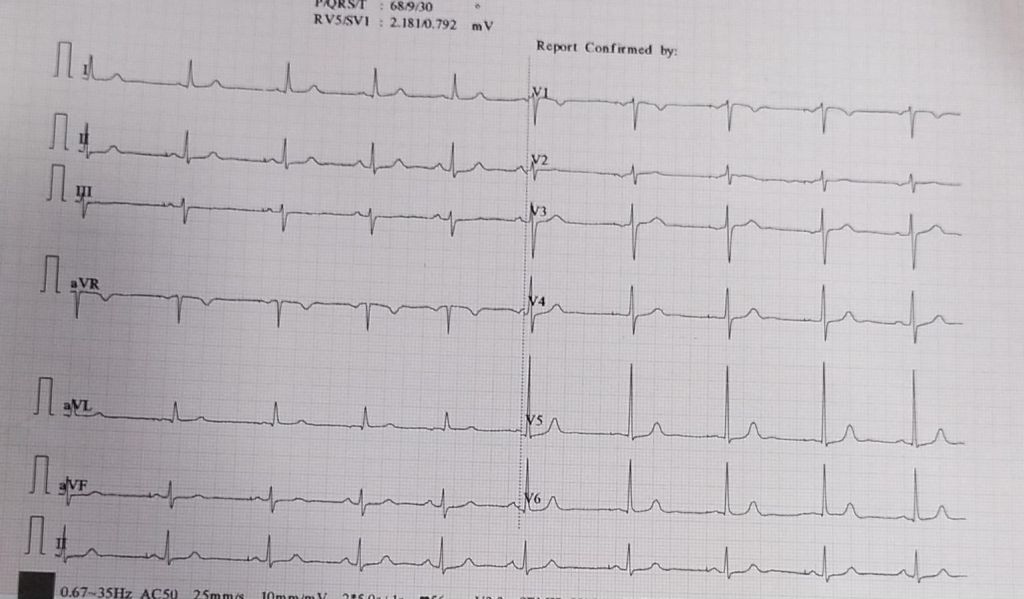
Answer : I think, we can’t answer this question with this ECG strip. So we can only guess it is DDD, as single chamber AAI pacemaker is not in vogue , even though it is the most physiological pacemaker possible in ideal conditions.( If any one has any points to differentiate , please comment)
* A pace V sense in DDD, though equivalent to AAI mode , can not be compared to AAI pacemaker, for the simple reason, ventricles just don’t have a lead in the later.
Final message
This post might appear as a EP parody. The purpose was different. It is sad to note AAI pacemaker might be dead , but the AAI as a mode will always be a great concept.It can beat on any day , the much hyped LBBBp in bulk of the pateints with SND in terms of physiology and synchrony.Fellows should realise single lead AAI can be most physiological , while, the DDD can become a pathological pacing , if it frequently switches to VVI mode , inspite of good AV conduction.
Part 2 :How do modern day DDD pacemakers reduce ventricle based pacing ?
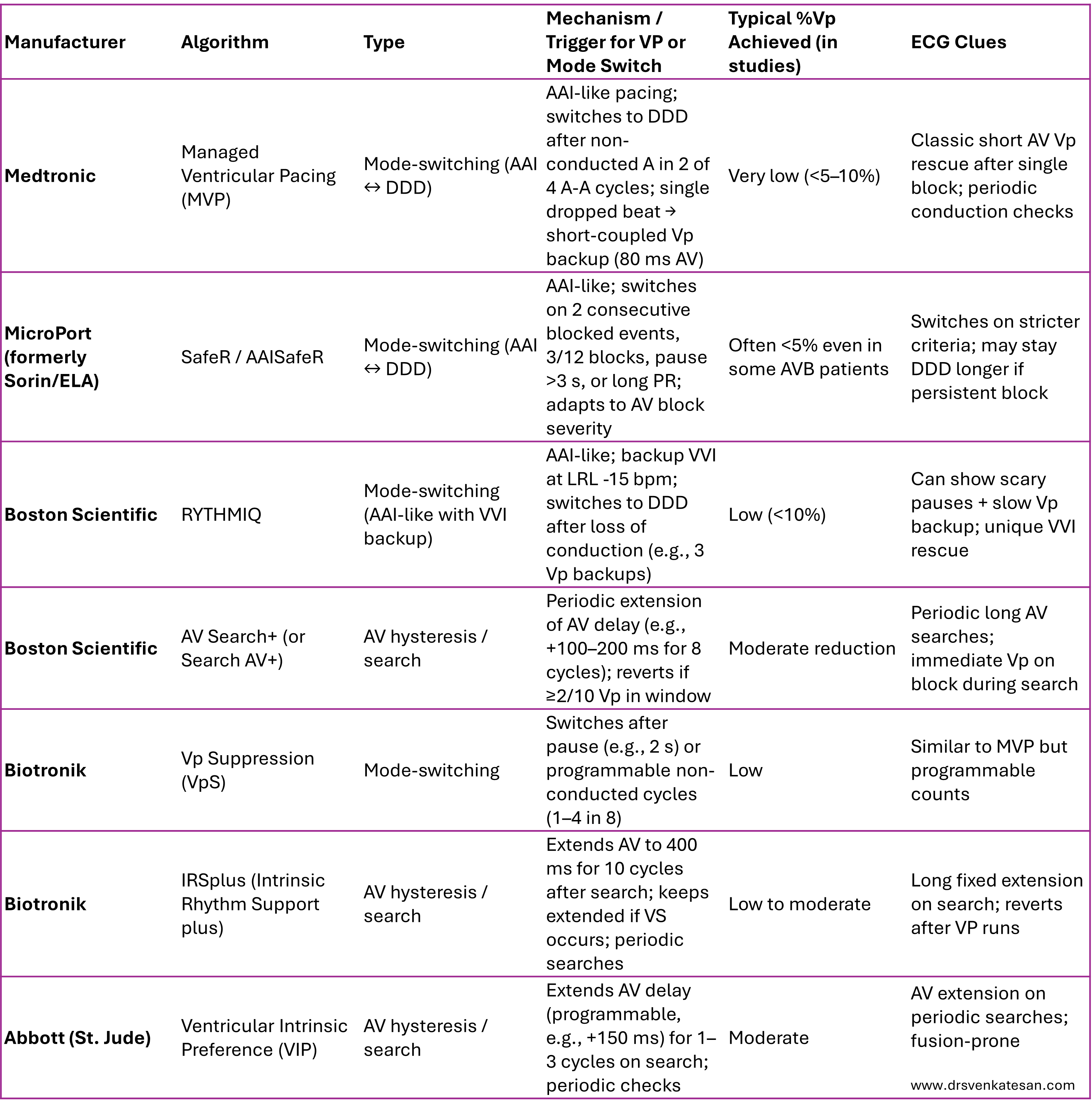
Pacemaker vendors have unique proprietary algorithms designed to minimize unnecessary right ventricular pacing (%Vp) while maintaining atrial-based pacing (effectively mimicking AAI/R behavior) in patients with intact or intermittently preserved AV conduction (e.g., sinus node dysfunction without significant AV block). These algorithms promote intrinsic ventricular activation to avoid dyssynchrony, reduce atrial fibrillation risk, and potentially improve long-term outcomes.
There are two main categories:
Mode-switching algorithms (AAI(R) ↔ DDD(R)): Operate primarily in atrial-based mode (AAI-like) with ventricular backup; switch to full DDD when AV block criteria are met.
AV hysteresis / search algorithms: Stay in DDD(R) but dynamically extend the AV delay to search for and favor intrinsic conduction.
Annexure : Company brands and different modes and algorithms (Compiled by Grok)
Getting a second opinion from another expert is a valuable option for our patients when they face a complex decision-making process, especially when a cardiac intervention is advised. No doubt, it is their fundamental rights too.But this could be hard, if the second opinion is sought regarding indication for coronary or interventional procedure.
It is much, much comfortable to concur with the original decision if it is pro -Intervention. (even if it is against your conscience). Vetoing a procedure which was advised by some big hospitals is almost impossible for cardiologists sitting at their office, however experienced they may be. This is because it is sort of going against, the mainstream and defying science as well. Both doctors and physicians are stuck.
I confront such situations often from patients following elite cardiology consults. I had been forthright and genuine and said a firm no or yes to many such procedures . I understood much later, that only a minority of the patients followed my No advice , while invariably they accepted my yes.
After much confabulations , recently, I have made some recalibarations on my values, (decent term for compromise ) despite all the ethical stuff I write in these columns. But, three things I ensure , before giving my opinion which goes against my assessment.
“This procedure is not indicated in the true scientific and moral sense, but 1.If you lack full trust, or 2. If you are not ready to accept the risks of not doing it, or 3. If the fear (of not doing it ), would nag you constantly, then get it done as per the advice of the big guys”.
Final message
Until we acquire the courage to express our true opinion , we certainly fall under the tag of medically incompetent.
Very soon, getting a second* or even third opinion may not really matter. Doctors are silently persuaded to follow the guidelines thursted by big scientific syndicates along with compulsion to go with patient wish & preference.
*Caution and clarification
Second clinical opinion for helping to arrive at a medical diagnosis is of immense value and a great thing to do. In fact, doctors themselves ask for it when they are in doubt. This article is about second opinion regarding the appropriateness of various interventional procedures that is defining modern medicine.
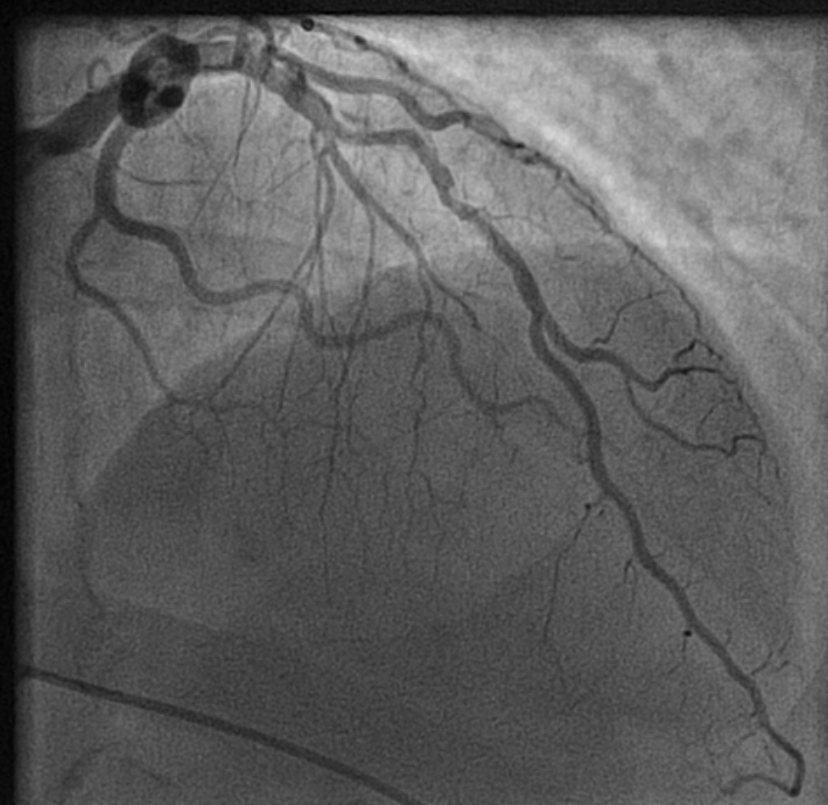
Decision making for PCI in chronic CAD continues to be delicate. This is especially true, if the lesion is Intermediate and the plaque vulnerablity is susepcted.
How to tackle this stress positive Intermediate LAD lesion. Functional capacity good. Non-diabetic, mildly elevated lipids. Now, continuing medical management with intensive lipid control is the best possible management. (We have evidence for medical management being good even in significant 90% lesion) Above is a case report from https://www.acc.org/education-and-meetings/patient-case-quizzes/medical-therapy-for-cad
Reassurance is a revascularization equivalent
Sharing a similar experience with one of my patients in his early fifties. After getting a fairly convincing consultation, he accepted medical management. However, guided by both NI & AI, he sought a second opinion to confirm whether my assurance was indeed correct. He underwent FFR and OCT, and both he and his plaque became vulnerable. The FFR was normal. He was too intelligent to ask about the FFR – Stress test discordance, for which his cardiologist had no answer. Still, they did not advise a PCI and the decision was left to him, respecting the current patient-oriented guidelines.
The patient went home empowered but spent sleepless nights, fearing about potential fissures, in the life sustaining fibrous cap.He believed that he was at the mercy of a 75-micron thin cap covering his plaque. In one of the anxious days,in the following week , he got admitted himself in a posh downtown cardiac center. A as per the guidelines, the patient chose his own pathway for a PCI. Cardiologists obliged piously to his wishes. Now, he feels better. He says he is happy to undergo a self prescribed stent.
I was glad, he had the courtesy to come back and showed the results. I learnt. it costed him 6 Lakhs and his insurance covered it fully. I realised , my 30 minutes reassurance was busted by the insurance card in few minutes. I wasn’t surprised.It’s okay, it’s all in the game. I learned it long ago. Fear* (either spontaneous or induced), the power to decide & affordability are the most powerful determinants of any inappropriate medical procedure.
Learning cardiology from UN & WHO
We have United Nations and WHO, the two global guardians. Any one with average intelligence will agree, these instituions can never bring either peace or health to this world.Let us ensure, the practice guidelines of cardiology doesn’t go that way. We boast ourselves, that we have a strongly evidence based vigorously scrutinized cardiology practice framework. How true it is ? Are we hiding behind pateint preference, and pushing science to the background ? Let us be transparent. I think it’s time, the powerful bodies like ACC/ESC should connect all the missing dots. .One important issue is, fear or anxiety-driven PCI, which usually overtakes other true indications.
Final message
In an ideal world , reassurance and GDMT , if properly done, should be a revascularization equivalent in most CAD patients .The reality is, fear* prevails over reassurance, for a variety of reasons.
Postamble
*Anxiety thrives well, in an environment of uncertainty. It is mutually inclusive among both patients and physicians.However most Professional physicians are expected to tackle it. Still many struggle. Patient : What if the block worsens? Physician: What if the patient comes back with an event and oh .. my pride and practice? May be, physicians are not to be blamed much. I think. it is all about a unexplained, biased human mind set. Even a death during an inapproproate Intervention is pardoned off, but an error, raising out of an appropriate medical mangment is rarely forgiven.
How many lives are saved by ECMO in refractory cardiogenic shock following STEMI ?
A. Substantial
B. Many
C. Atleaset few
D. None
E. It may even Increase the fatality
Answer
While the popular answer swings between A to D , depending upon the level of optimism & belief system of cardiologists.
However, the correct answer is likely to be D(Ref 1) .
*While C, is quiet possible, E is very much a reality all experienced cardiologist would know.
Postamble
* My non-academic opinion is, ECMO and other MCS devices, are primarily, “guilt-relieving or professional pride delivering” toolkits for the patient’s family and cardiologists, respectively.
This is a very crucial question debated, by cardiologists , cardiac surgeons for long decades (of course our patients too need an answer desperately)
Will CABG prevent or reduce future MI risk ?
The answer is not at all simple , most of us are still tentative.
Have a look at the conclusion of these two famous studies. STICH and STICHES. Hope, we could reach closer to a clear answer.Ofcourse, the study population may not fit in to all the CAD population we come across. Still, it conveys some useful information about this issue.
Final mesage
It is indeed true a STICH in time , really saves nine.
Postamble
The toughness of answering this question lies in the fact, it takes hardly three minutes , for a non flow limiting 30% lesion to transform to a life threatening ACS.
Real world data reveals, most patients with multivessel CAD harbor, a minimum of half a dozen non flow limiting lesions. CABG has a huge edge, in this situation ,as most of these lesions are proximal to bypass conduit.
Counter point
Lastly , and most importantly, it is the intensive medical management and life style modifications, that will determine, whether CABGs are going to work, as it did , to the lucky patients of STICHES cohort.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.