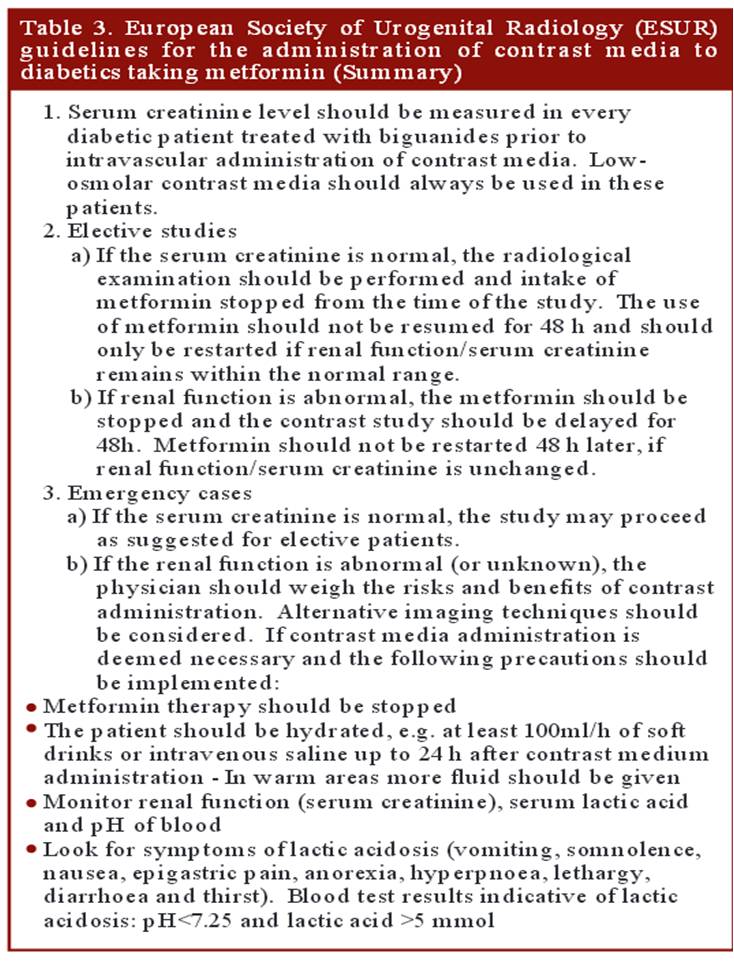
Metformin is one of most commonly used oral hypoglycemic drug listed by WHO as an essential anti diabetic drug. .It is a biguanide which blocks the hepatic gluoneogenesis . Since lactate is the major substrate for the process of gluco-neogenesis , excess of which spills into blood .Lactate is swiftly cleared by the normally functioning kidneys .Metformin is completely excreted by the kidney. Hence in patients with compromised renal function (or when contrast agents compete with Metformin in renal excretion ) high levels would not only cause lactic acidosis (> 5meq), it can also aggravate contrast induced renal injury resulting in a downward hepato -reno-metabolic spiral.
Though the incidence of Metformin induced Lactic acidoss is low , the outcome can be bad , hence the concern. The European society of urogenital radiology has provided clear cut guidelines regarding Metformin usage when contrast agents are being used.
What can be done in emergency situations
- Since the risk of lactic acidosis is very low , in case of emergency situations Metformin need not be discontinued prior to contrast usage.However it need to be stopped for 48 hours from the index procedure. (Fortunately Metformin is a dialysible drug that can be removed in case of toxic accumulation.)
- Consider alternate mode of Imaging if renal function is really concerning
Reference
2. http://ccforum.com/content/pdf/cc12886.pdf
A good article from drug review Contrast induced nephropathy and metformin






{kind=link}