Co-dominant coronary circulation is defined as , when posterior crux of the heart receives twigs from both right and left system making this water shed area with advantage of twin innervation.They essentially supply inferior and posterior aspect of both left and right ventricle including the posterior aspect of interventricular septum.
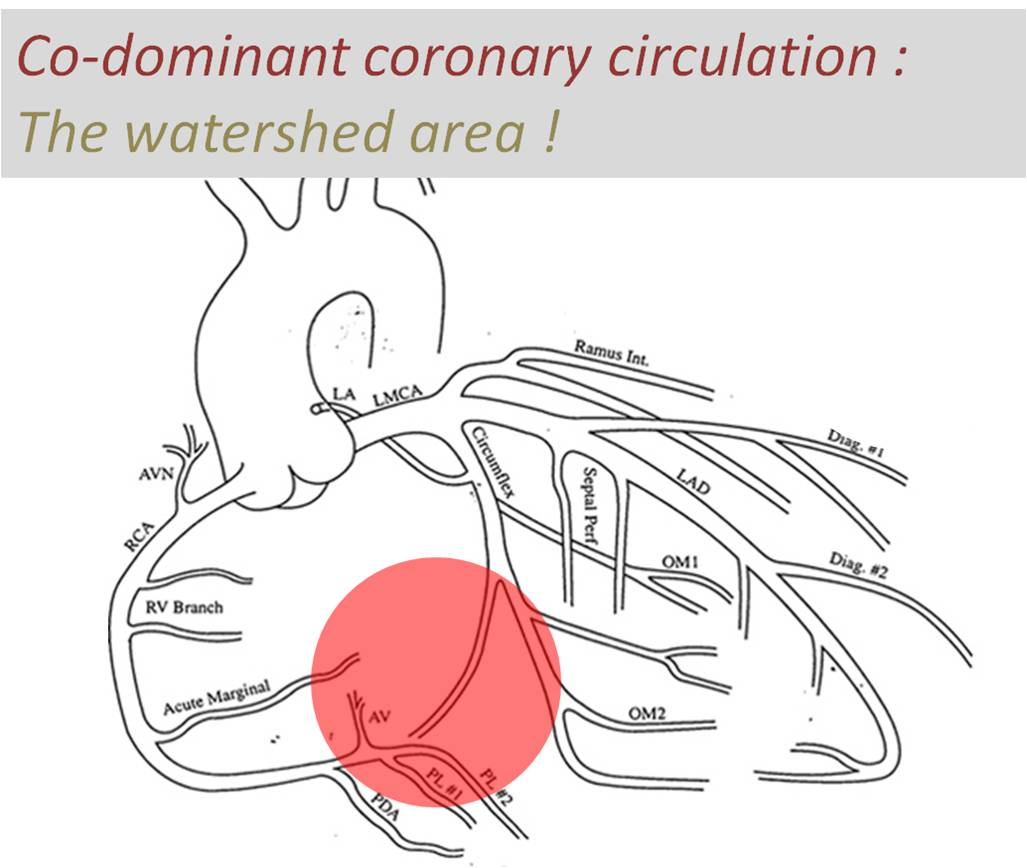
Image courtesy modified from :http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/image4.JPG
Traditionally inferior and basal aspects of heart are perceived (wrong tough !) as less important than anterior surface of heart.Infero posterior MI can be extensive and cause significant LV dysfunction and poor outcome. Longitudinal function (AV grooval velocity) and Mitral valve function is critically dependent on posterior circulation.
Is there an advantage for co-dominant circulation with reference to ischemic mitral regurgitation ?
Obviously ,one would expect there is some advantage in co-dominant circulation when ACS occurs either LCX or RCA.It could theoretically protect against development of MR as posterior papillary muscles could receive supportive twigs from its companion.
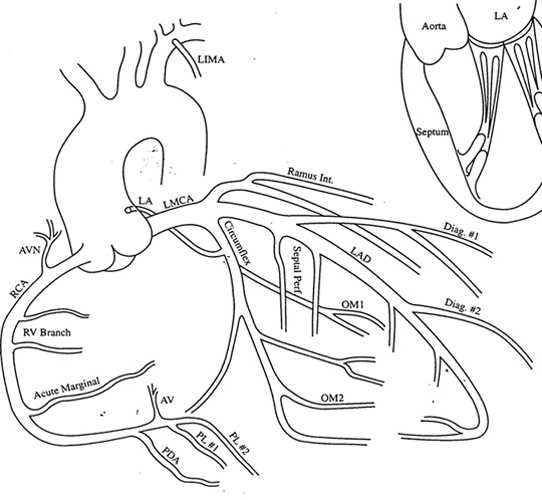
However , there is a caveat .The antero-lateral papillary muscle normally has twin blood supply from LAD(Diagonal ) and LCX (OM) . But in co-dominant circulation this pap muscle is at risk of becoming single blood supply as the dominant RCA has a trade off with OM with its large PLV branch. It is likely in co-dominant circulations if LAD is the culprit outcomes are likely to be worse.
Final message
A rare study involving more than 200,000 patients which specifically addressed this issue of dominance and outcome , threw some surprising findings. In concluded PCI outcomes with left or co-dominance has a worse outcome than Right dominant system.
Reference
2.Papillary Muscle Perfusion Pattern A Hypothesis for Ischemic Papillary Muscle DysfunctioPaolo Voci, Federico Bilotta, Quintilio Caretta,Circulation. 1995; 91: 1714-1718




{kind=link}
Leave a comment