Wall motion defect , in patients after CABG is fairly common.These defects are difficult to interpret as the mechanisms can be multiple.Though the commonest wall motion defect appears to involve the interventricular septum. it can occur anywhere in antero-lateral zone.
The mechanism attributed is the effect of pericardiotomy , which surgeons as we understand leave it open after grafting .This can cause lack of localised ventricular interdependence and results in a a brisk septal movement (bounce )It is an indirect effect .
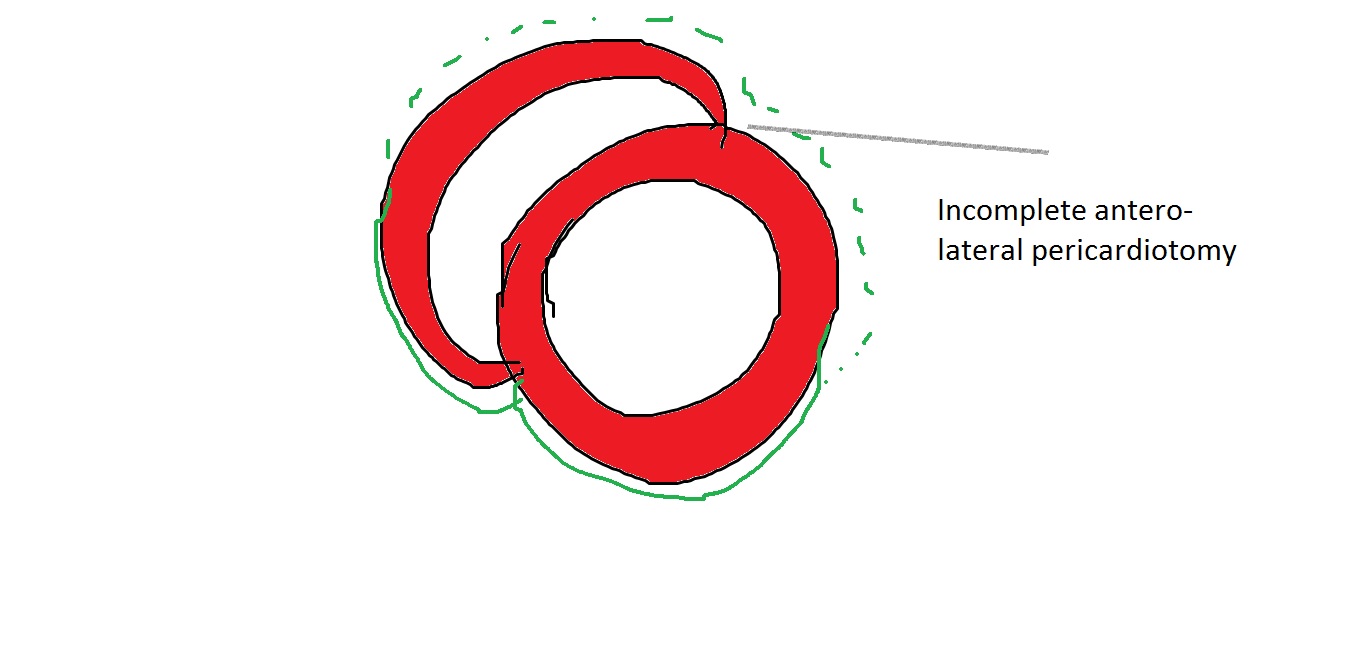
Note the, wall motion defects are confined to the exposed areas of the heart during cardiac surgery .In short axis echocardiography it correlates anywhere between 9 to 3 O clock position. Though interventricular septum is not covered by pericardium in the true sense , there is a indirect bounce effect over IVS due to interference with anterior ventricular interdependence .
More commonly a direct wall motion defect in the 12 to 3 O clock position in short axis is seen .This can closely mimic true wall motion defect as pericardial adhesions can tether these segments. Careful observation is warranted.Myocardial thickening is the key differentiating feature.
What is the physiological impact of these wall motion defects ?
It is generally considered benign (It is !) .Though in echo it looks awkward and suggest desynchrony. The real issue is , it can mislead the echocardiographer to errors in calculation of that universally sacred parameter called EF %
Importance of knowing pre existing wall motion defect.
This has to be reviewed with old reports as it can wrongly create a new wall motion defect de-crediting the surgeons.
New pathological wall motion defect.
Of course it can happen due to peri-operative ischemic insult or infarct . However , It need to emphasised transient wall motion defects are common post CABG due to apparent hypoxia.This seems to be more pronounced with on pump surgeries than off pump .(Expected though) In my opinion, 2-4 weeks cooling off period is required before a meaningful assessment of wall motion post CABG.
Late pericardial reactions and localised constrictive features has been reported.
Disappearance of wall motion defect : How common ?
Any disappearance of WMA is welcome . It happens rarely though . Some of the post ACS population (Both STEMI and UA/NSTEMI) can experience this , as they could harbor zones of myocardial segments afflicted by ischemic stunning rather than true necrosis , that might disappear.




Leave a comment