A 50-year-old man was referred for dizziness, bradycardia and dysphagia .He was very clear in describing his symptoms and landed up in Gastro- enterology OPD , from there was referred to my clinic for cardiac work up . His ECG showed a sinus bradycardia HR of 48 /mt.
Echocardiogram revealed a structurally normal heart as we expected , but was surprised to spot suspicious shadow in para-sternal long axis view , beneath left atrium.
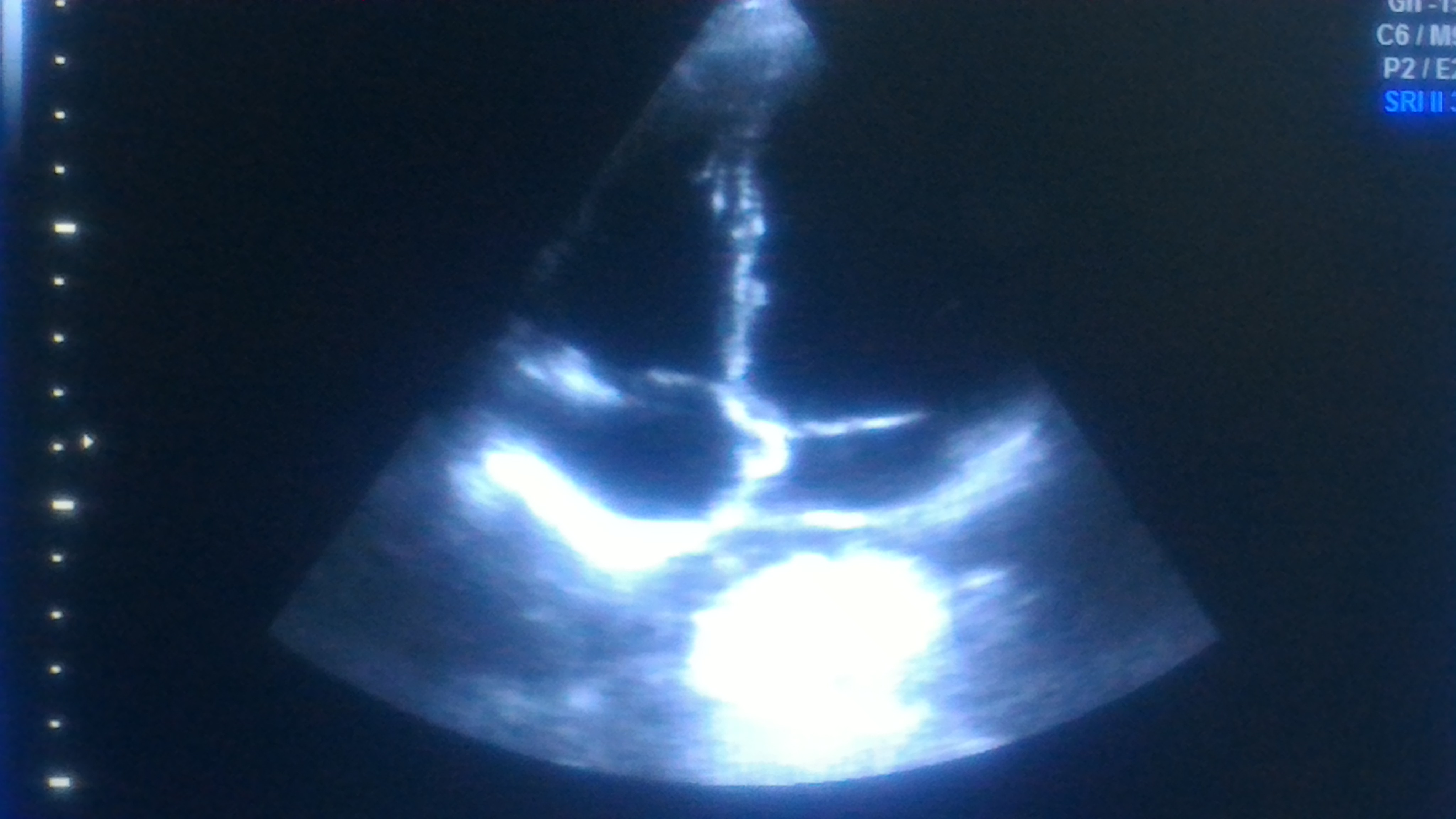
A well demarcated large mass compressing left atrium. Trans Thoracic Echocardiography may not be looking at the heart alone ,(Its technically Thoracic Ultrasound though we may refer it as Echocardiogram )
- Aortic aneurysm ?
- Mediastinal teratoma?
- Bronchial adenoma ?
- Esophageal mass ?
The Answer is none of the above
As I was wondering what it was, the staff nurse in charge threw a heavy folder with well worked up gastro Investigations.
That moment , diagnosis became obvious , without a need for further scrutiny to my medical acumen.

Note: The barium swallow of the Esophagus reveals the Intimate relationship between the food tube and the heart as it descends vertically downwards posteriorly . Realise , how the proximity of these two structures could confuse a physician when symptoms spill over on either way. (I would have expected a lateral view to show the compressive effect of Esophagus on the left atrium the radiologists felt its not important !)

Yes , it is Achalasia of the cardia , dilating the lower end of esophagus with fluid /mass effect , compressing the posterior surface of Left atrium.He underwent a myomectomy surgery.
Why bradycardia ?
There is well described esophago-vagal reflex reproducible by stressful swallow or balloon inflation in the lower end of esophagus at D7 level.(Ki Hoon Kang,Korean J Intern Med. 2005 Mar; 20(1): 68–71.)
Achalasia cardia is known to be associated with symptomatic bradycardia, dizziness, and rarely swallow syncope,though this patient didn’t have a classical syncope.The bradycardia is probably due to high vagotonia, (Hugging effect on posterior surface of heart known for rich innervation of vagus.) . Complete reversal of bradycardia after esophago -gastric surgery is expected.
Implication for cardiologists
There has been instances of patients with esophageal syncope and reflex bradycardia getting permanent pacemaker therapy. I think , clinical or sub clinical esophageal disorders should be included in the work bradycardia before labelling them as intrinsic sinus node dysfunction .(Ref 1,4)
Final message
The field of Cardiology is often referred to as a super specialty atleast in India . I disagree with it strongly. Cardiologists are neither super(eme) nor special .We need to be reminded its afterall a sub-specialty of Internal medicine and each specialist should undergo retro-training in medicine periodically .This patient is a typical example of a gastric problem entering the domain of cardiac Imaging.Strong foundations in symptom analysis and some degree of medical curiosity will enable an occasional cardiologist to make a correct diagnosis belonging to a remote foreign specialty.
Reference
1. Palmer ED. The abnormal upper gastrointestinal vagovagal reflexes that affect the heart. Am J Gastroenterol. 1976;66:513–522. [PubMed]
2.Armstrong PW, McMillan DG, Simon JB. Swallow syncope. Can Med Assoc J. 1985;132:1281–1284. [PMC free article] [PubMed]