The right ventricle is considered as a docile cardiac chamber with passive filling and emptying properties .
This belief was reinforced when Fontan in early 1970s suggested a principle in the management of cyanotic heart disease when the right side of the heart is underdeveloped. He proved RV can be by-passed safely , with great veins (IVC/SVC) by themselves take care of filling the pulmonary circulation without the need of RV pumping function.
While it is true for few complex cyanotic heart disease, largely this a misleading concept. In clinical cardiology practice ,sudden or non sudden RV deaths happen every day in the form of . . .
- RV Infarction
- Acute RV dysfunction in massive pulmonary embolism
- COPD with RV dysfunction
- Most cases dilated cardiomypathy the terminal event is due to RV failure.
So , RV function can never be dispensable in day to day cardiac hemodynamics.
RV has some unique properties in terms of shape , size and hemodynamics . We are getting more insights from modern blood pool imaging by MRI , about how the RV handles the blood volume .
We know RV has a unique shape triangular ( partially pyramidal ) . It can be inferred the RV cavity is formed by fusion of many eccentric spacial planes. We have always believed RV handles the blood it receives from right atrium in a unique way .Now we are beginning to understand it .It is now documented the RV segregates the blood it receives into 4 components.
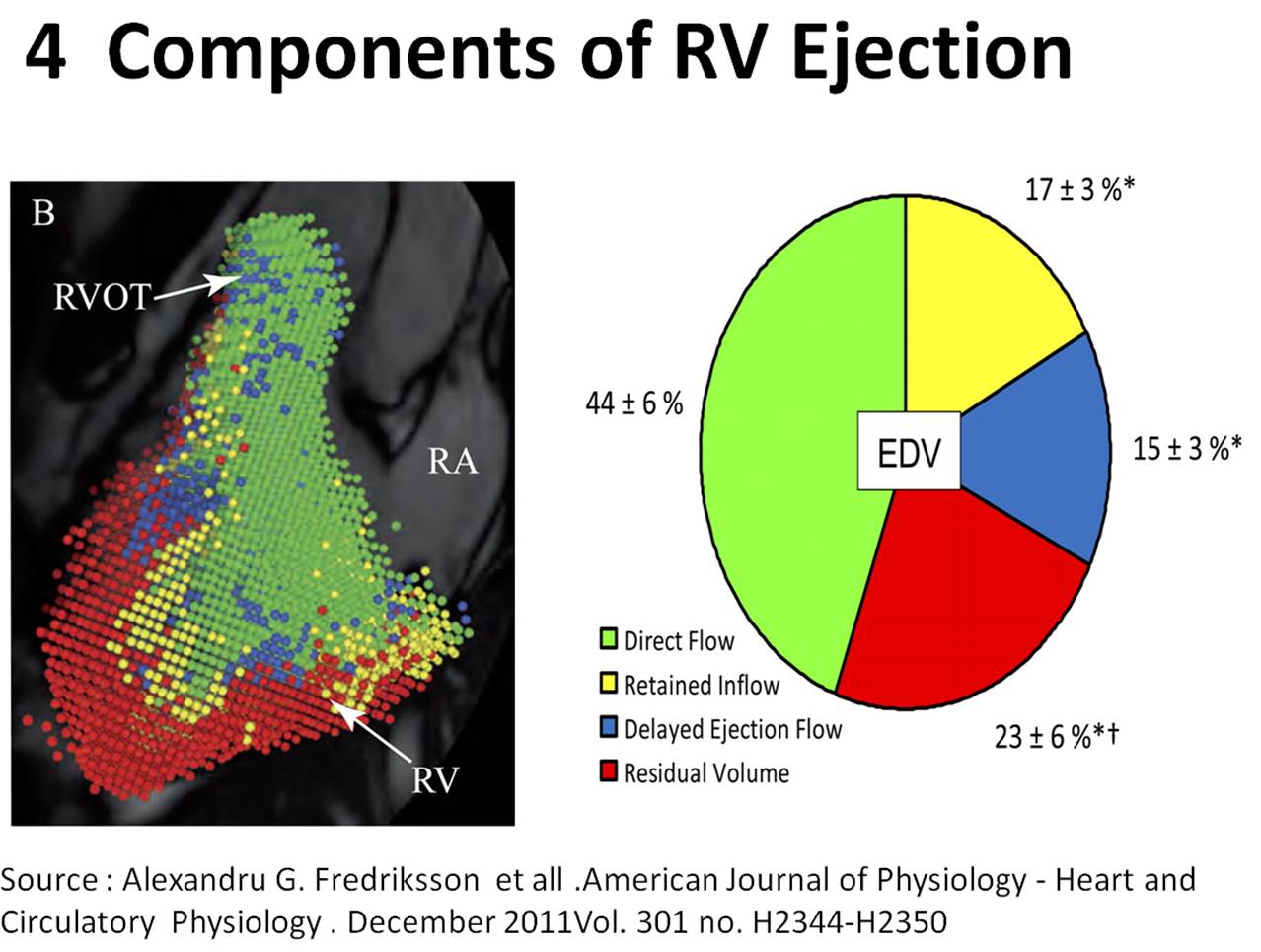
It is curious to know RV inflow is connected to the outflow by an invisible physiologic Bridge . About 44% of blood traverse the RV in this fashion.
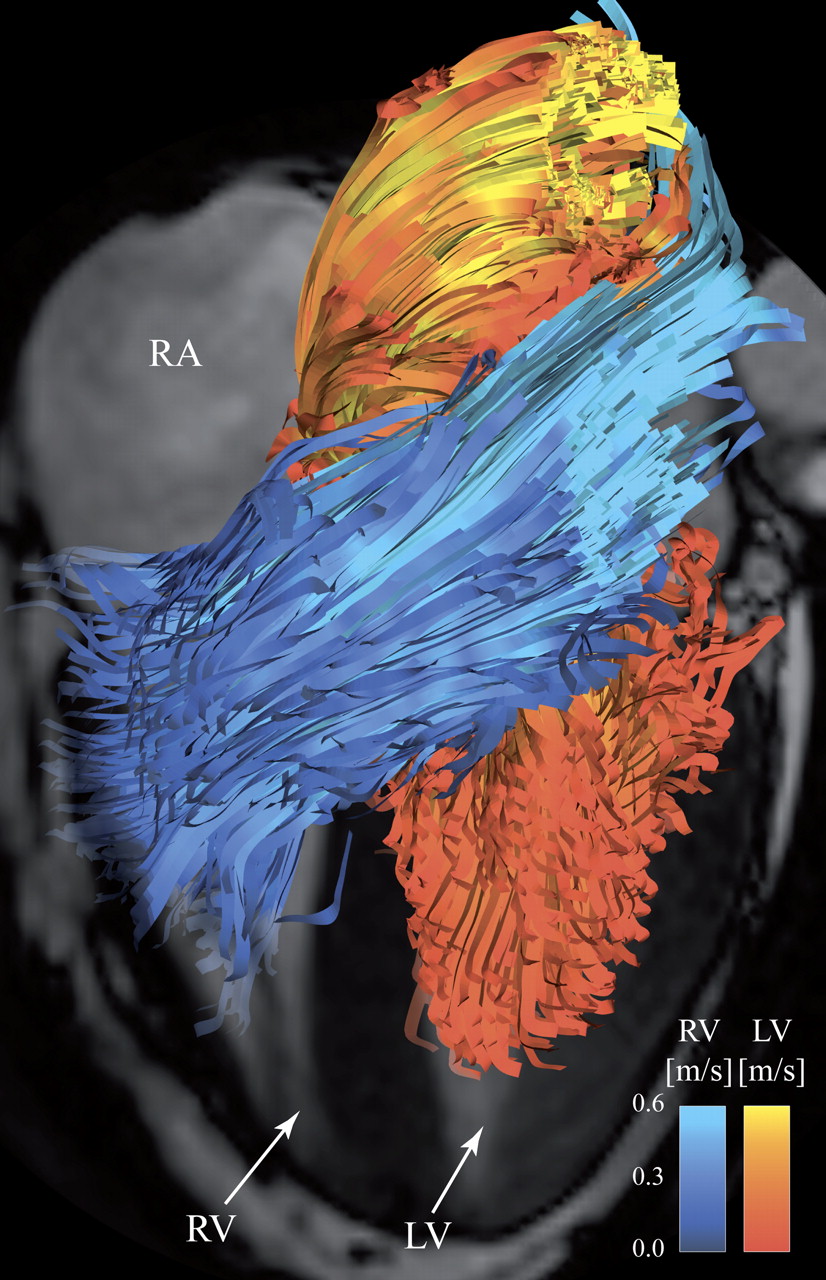
Note : RV blood flow preferentially enters the RVOT with out transiting RV body and apex.Image courtesy http://ajpheart.physiology.org/
Which is the most important part in RV ? (Among Inflow, Body, Apex, Out flow)
After reading this article it seems to me , the mechanical function of RVOT could be most vital. If it fails to handle the first increment which comes directly from RV inflow, stasis is likely in RV body and apex , elevating RVEDP and later promoting stasis leading to clinical events.
Clinical implication of this study
- Differential dilatation RV chambers to pressure or volume overload is observed .
- We need to analyse why RV dilates in some but goes for hypertrophy in others when confronted with pressure overload (VPS vs PAH)
- RV apical clot in restrictive cardiomyopathy is a direct consequence of stasis of blood in RV apical zone .
- RVOT pacing may have a hemodynamic advantage over RV apical pacing . However , for anatomical reasons RV apical pacing is far safer than RVOT pacing where the lead is subjected to constant life long strain due to this busy RV inflow to outflow express high way !
Final message
Traditionally we have labeled RV as a passive venous chamber .It is clearly a misnomer.It has to handle both the venous and pumping function beat to beat with precision without back log .Obviously , RV has to think and work more than it’s big brother !
Reference
I wonder , if there is any other site other than APS . . . to find crucial answers in cardiac physiology !
 After thought
After thought
- There is huge gap between physiologists who work in research labs and the physicians at bed side .
- I appeal all young cardiologists to visit APS once in a while ,between your busy cath lab schedule and help narrow this gap.
- Without understanding the physiology properly how are we going to intervene the pathology ?



