The cell of origin of ventricular tachycardia is rarely discussed at bedside. It is still in research labs !
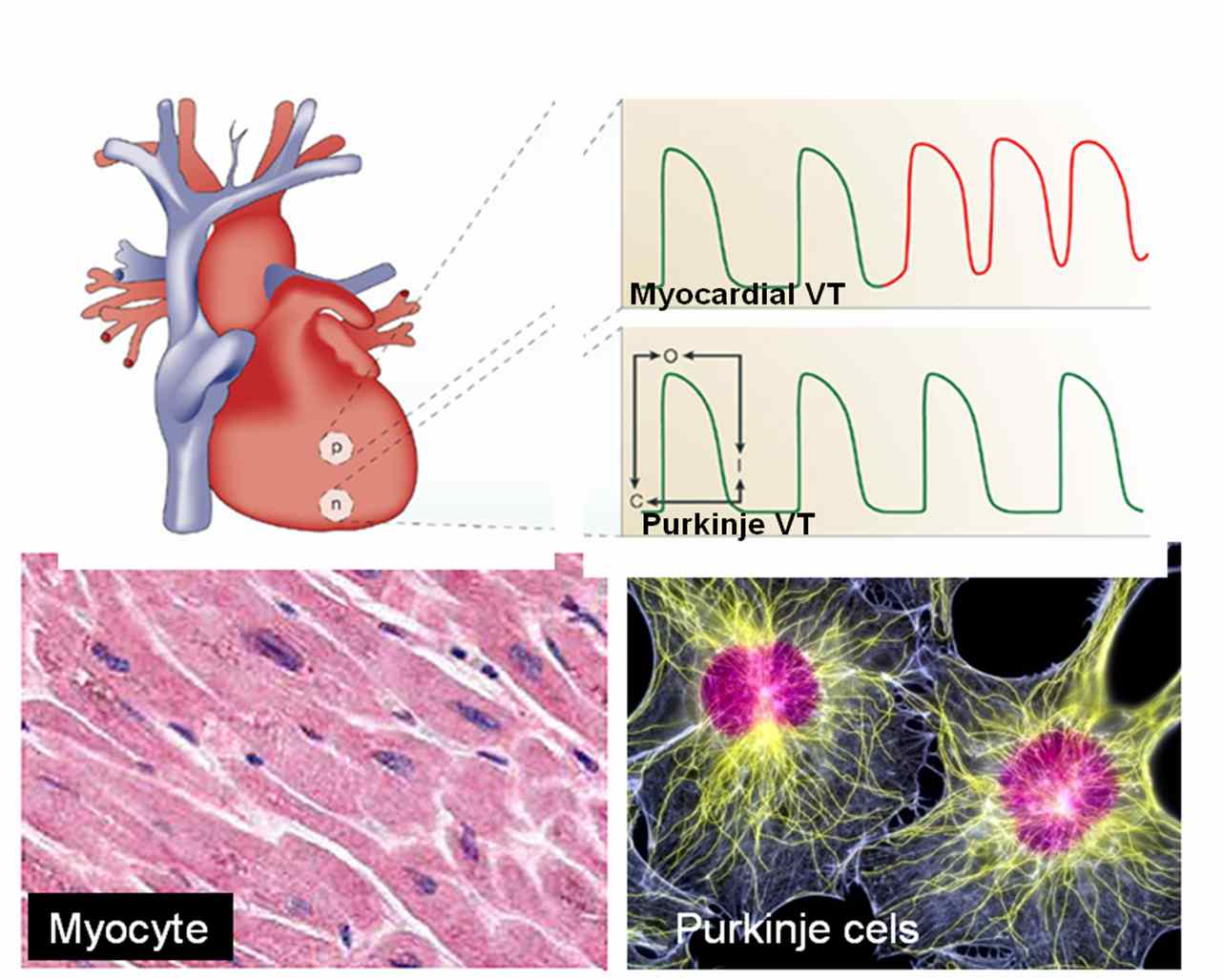
Ventricles are not made up off entirely myocytes. Apart from myocytes it contains specialised purkinje cells , fibrocytes, interstitial cells and some times primitive mesenchymal cells. Ventricular tachycardia can arise either in purkinje cells, the myocytes or even the fibrocytes. The myocyte VT classically occur during ACS or post infarct VTs.They are more often hemodynamically unstable and quickly degenerate into ventricular fibrillation. Myocardial VT is likely to be pulseless and require DC cardiversion frequently. Purkinje VTs are relatively less unstable. If VT arise proximally in the septum near the distal his, or in bundle branches (BBR) the VT is more stable.They are likely to respond to be medical management.

What is the therapeutic implication of knowing myocardial VT ?
In fact ,simply knowing the cell of origin of VT is not suffice .The ionic currents inside the cell that trigger and sustain the VT is more important. There are few ionic circuits responsible for VT. Sodium , Intra cellular calcium, potassium , beta receptor mediated calcium current.If we know the individual ionic culpirit we can block that specifically . Now we have multi purpose ion blockers like amiodarone which acts like a broad spectrum antibiotic and terminates a VT.
So as of now there is no real purpose of breaking our head in locating the cell of origin and the ions responsible for VT at the bed side ,( Researchers will do that for us !). We have only few antiarrhythmic drugs available in our crash cart .Our job is to choose the optimal drug which will fit in for our patient. In electro physiology labs, radio frequency ablation is done .This is nothing but shooting down the abnormal electrical focus (Cluster of cells or a samll segment of myocardium). In future, a single abnormal cell could be selectively neutralised with cell based therapy assisted by nanopore robots !




{kind=link}
Leave a comment