This is not a breaking news story. It’s the same old secret that was exposed in JUPITER trial with Rosuvostatin 14 years ago. Yes, I am talking about the relationship between the usage of statin and the occurrence of diabetes. Now, we have this huge study on possible diabetes progression with statins. It’s not from a small journal to ignore.
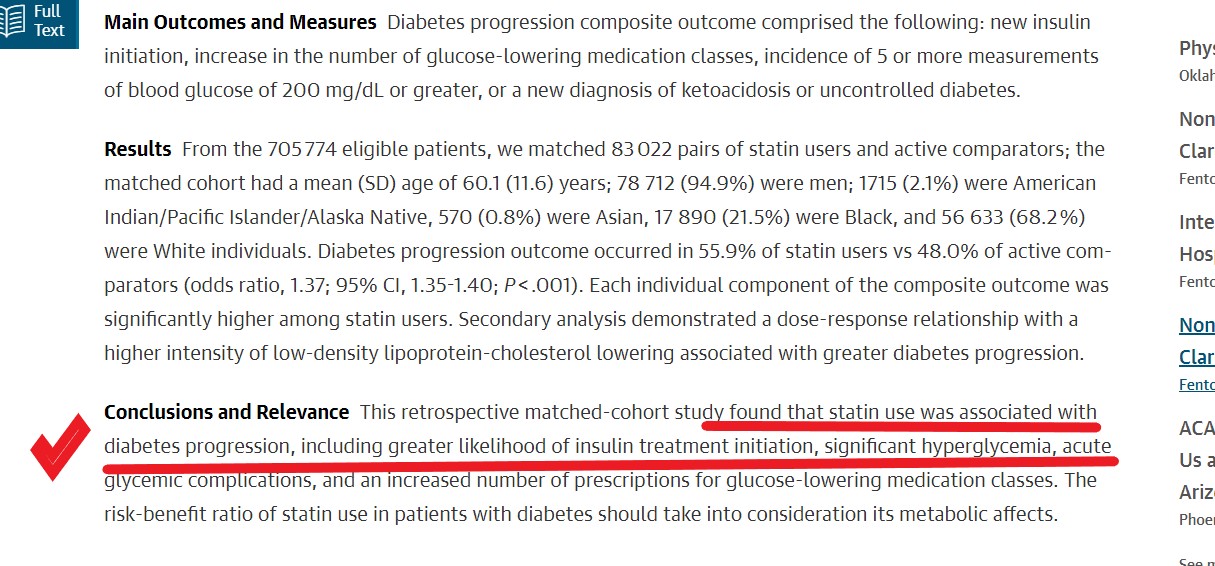
83 thousand patients data, the world’s largest series on link between statin therapy and diabetes.
This study has this to conclude
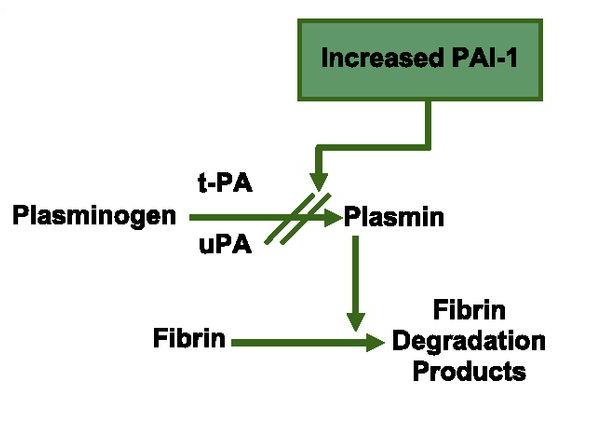
Diabetogenic statins
Something* happens as the statins antagonize the HMG COA enzyme that resides within the delicate membranes of the endoplasmic reticulum inside the most specialized cells in our human body, called hepatocytes.
*What is that something?
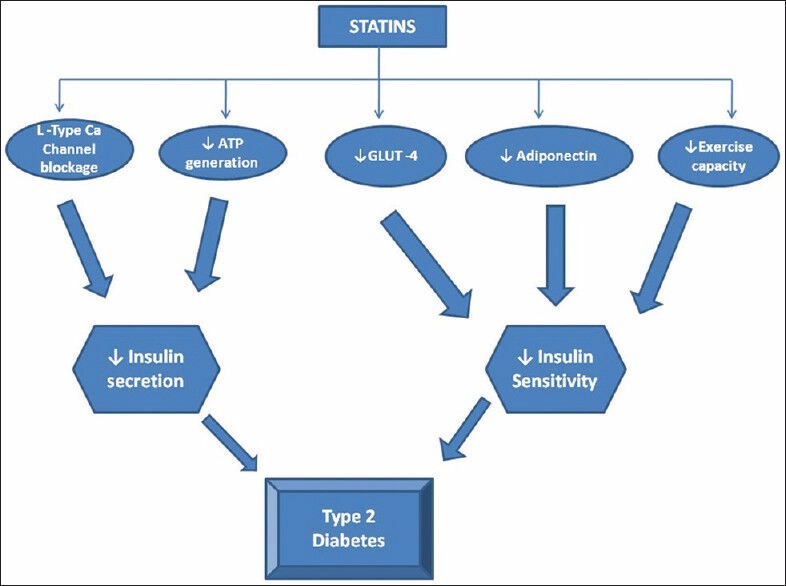
Image source Umme Aiman et al Journal of Pharmacology and Pharmacotherapeutics 5(3):181-5DOI: 10.4103/0976-500X.136097
How to go about this issue?
With-holding statin in as many as possible is the best thing for such diabetic (non-diabetic?) patients. But, the more pragmatic option is to ignore these negative studies, and instead intensify diabetes management if it worsens. After all, we can’t afford to lose the prodigious evidence-based cardio-vascular protective effects of statins and earn the wrath of our patients and peers you know!
Further Interest