
Posts Tagged ‘evidence based medicine’
Evidence based common sense, is rare entity in medical literature
Posted in Uncategorized, tagged bmj, common sense in medicine, ebm, ethics in medicine, evidence based medicine, experince based medicine, false evidence, jacc, jama network, lancet, medical education, nejm, pitflls of ebm on July 10, 2025|
A forgotten job function of a Physician
Posted in Uncategorized, tagged ethics, evidence based medicine, medcial education, peer reviewed journals on December 11, 2024|
False enemies in medical practice
Posted in Uncategorized, tagged drs venkatesan, ethics in medicine, evidence based medicine, experince based medicine, hippocrates, madras medicalcollege, principles ofpracticeof medicine on November 9, 2024|
Will meta-analysis really come under an original scientific research ?
Posted in Uncategorized, tagged evidence based medicine, fisher, jama network, journalof statistics, kaplan meir, lancet, levels of evidence, medical ethics, medical statistics, MEDICALEDUCATION, meta-analyses, meta-analysis, nejm, pearson, pvalue, randomised control trial, rct vs metaanalyses, why two meta analysis difer ? on October 10, 2024|
“In one sense, meta-analysis would come closer to a milder form of ethical plagiarism”
Can meta-analysis really be called as original scientific research ?
No it is not, but some may say yes. It is very difficult to dispute either. But, the fact of the matter is, meta-analyses are not a true science of innovation. It is using some others’ work( sort of intellectual steal ?) done by a group of scientists interested in the same research topic, trying to squeeze more info from these studies. It is a glorified group journal club activity.
Image source & Courtesy http://www.inquasar.com
At best, meta-analysis can be referred to as knowledge and evidence aggregation. Surprisingly, mostof the academia seems to give more weight to meta-analysis, disproportionately more than the original researchers. This is because meta-analytic scientists backed by big journals claim, they can bring out more info out of the original. The assumed scientific superiority of meta-analysis is expected to be downgraded soon, as these sort of evidence aggregation can be done easily by any AI-powered engines. Network meta analysis, by dedicated medical scholastic AI networks can do this in a fraction of a second.
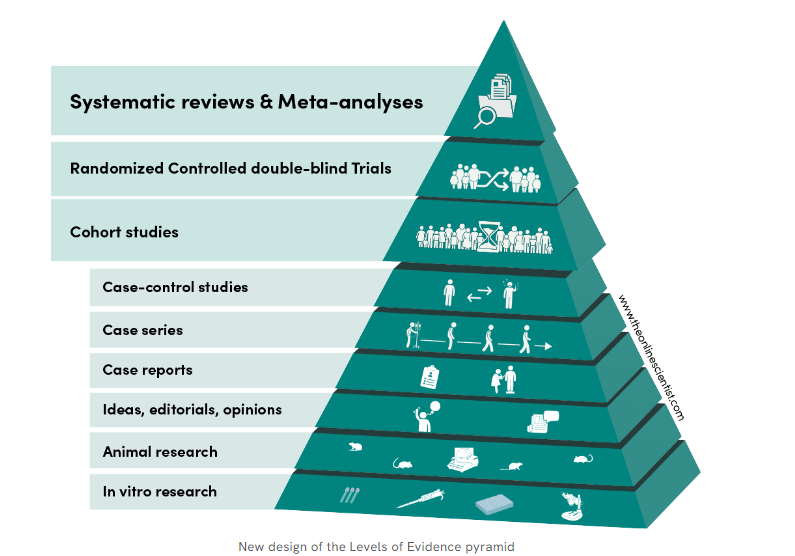
Meta analyses as of now is sitting proudly as crowning glory at the top of evidence pyramid. This is one of the reasons for the false glory surrounding anyone (or anything ) associated with meta-analyses. I doubt whether it really deserve the top slot. (An excellent debate between RCT vs metanalysis) Wish, the meta-analysis taste its own medicine at least once. We need to have a meta-analysis to show it is really superior to other forms of evidence. I cant find one as yet.
What about systematic review ? This looks better, as it has less statistical content , and the researcher is at least compelled to go deep and get enlightened on the topic as they spend months together on the topic.
How is meta analysis different from original research?
There is no new data collection ,no primary hypothesis testing . It primarily focus on summarizing existing evidence. To do it properly, there are certain standards.
- PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)
- Cochrane Handbook for Systematic Reviews of Interventions
- MOOSE (Meta-analysis of Observational Studies in Epidemiology)
Positive side of metanalysis
While meta-analyses aren’t original research, it’s a crucial tool for evidence synthesis, research translation informed decision-making.
Flaws of metanalysis
It is a academic business with done studies. So it is 100% retrospective. It might come with irreversible errors. Unless every error in the past studies is accounted for and curated the result of meta-analysis, it can never be foolproof.
Should we get permission from all the authors who did their original studies before doing a meta-analysis?
As long as fair use criteria applies there is no need , but a moral obligation is definitely there . Other wise metanalyses will come closer to a milder form of academic plagiarism of others’ work. (Of course legally and scientifically approved)
Final message
In the world of true scientific research, meta-analyses can not be considered as great scientific work. It is just evidence aggregation, which of course could be meaningful if and only if the studies taken were done properly.
However, meta-analysis has undisputed value in aggregating rare cases, scenarios, diseases, and problems where there are very few published studies. Collecting them together in an organized fashion serves a real good purpose.
Reference
1.Pearson K. Report on certain enteric fever inoculation statistics. Br Med J. 1904;3:1243–6.
A forbidden quote in medical science
Posted in Uncategorized, tagged empircal medicine, ethics in cardiology, evidence based cardiology, evidence based medicine, FAKE VS TRUE EVIDENCE, jama network, lack evidence, lancet, MBEST QUOTES IN MEDICAL ETHICS, MEDICALEDUCATION, nejm, randomised controll trials, venkatesan sangareddi on September 14, 2024|
When does a fact become an opinion & vice versa?
Posted in Uncategorized, tagged class c evidence, evidence based medicine, evidence vs opinion on October 11, 2023|
When we realise, even class 1-A indication often blinks at the bed side,while class III -C appear to pour more sense, practicing cardiology becomes "Tough and exhilarating” .
Testing times for EBM : NEJM gets ready & begins a new journey
Posted in Uncategorized, tagged bmj, ebm, ethics in science, evidence based medicine, lancet, medical education, nejm, new nejm journal on January 19, 2022|
The New England Journal of Medicine (NEJM) the premier journal in medicine originated two centuries ago, in 1811, when John Collins Warren, a Boston physician, along with James Jackson, submitted a formal prospectus to establish the New England Journal of Medicine and Surgery and Collateral Branches of Science as a medical and philosophical journal.
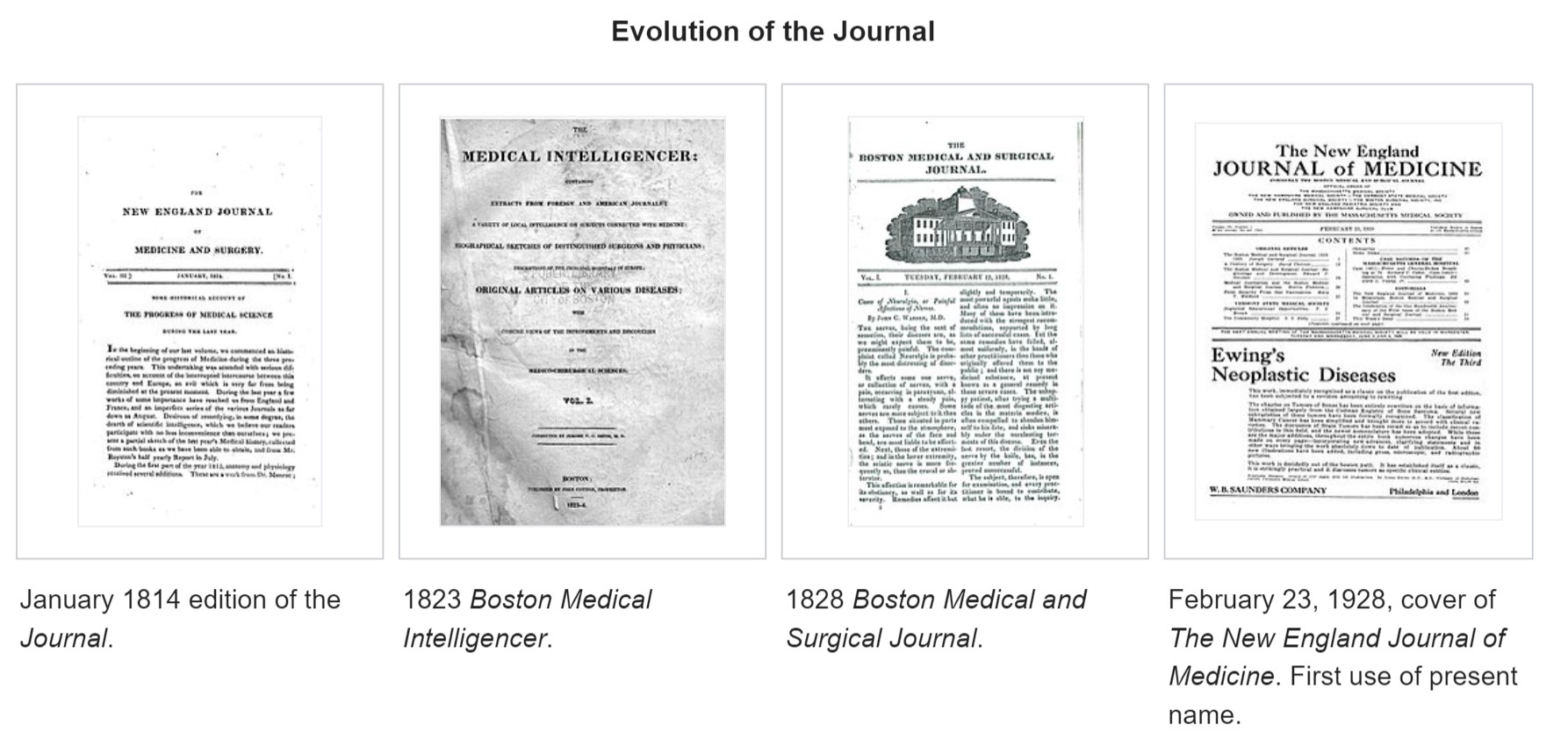
Subsequently, the Massachusetts Medical Society (MMS) purchased the Journal for US$1 and, in 1928, renamed it to The New England Journal of Medicine.
NEJM’s New Journey
It is 2022, after 200 years of providing explosive knowledge in medical science, MMS starts a new journal, fresh and bold. It is called NEJM Evidence. Can you guess, what is the need for such a journal now? I think the most battered word in science in current times is probably “ evidence”. It has a unique character of appearing most sacred as well as scandalous at the same time.
NEJM has remained the torchbearer of almost all advances in the medical field seen in the last two centuries. It is heartening to note the newborn is named as NEJM evidence. It has come at a critical juncture. I am sure, everyone will acknowledge that we are at difficult crossroads. Overwhelmed with unregulated scientific discoveries and publications, struggling to deal with self-inflicted knowledge pandemic. In the process, we have lost “not only” the ability to ignore trivial health issues “but also” failed to provide simple, cost-effective care to the real patients who desperately need it.
Let us hope, (& wish,) NEJM’s new prodigy will guide medical science towards a successful, meaningful, and ethically fulfilling journey for mankind. Meanwhile, let us pray for every medical scientist to be blessed with the required strength and courage to steer in the right direction, weeding off both academic and non-academic contaminants.
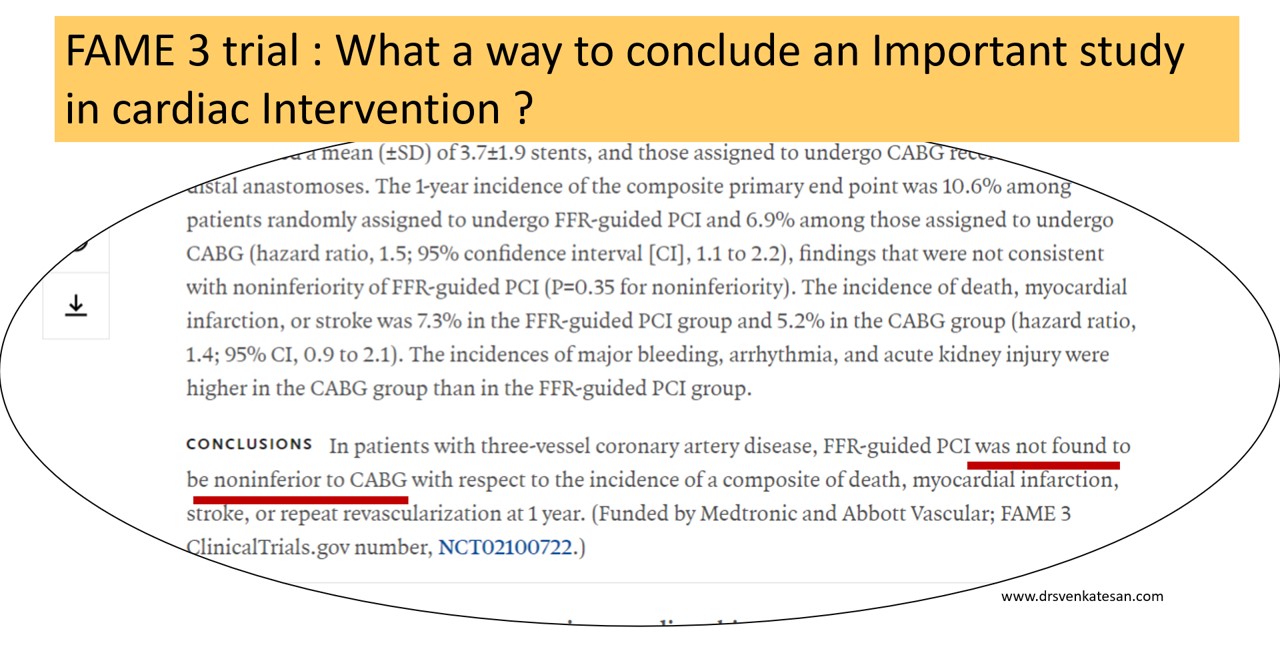
FAME 3 fails to defame CABG, cardiologists need not worry though !
Posted in Cardiology -Therapeutic dilemma, Cardiology -unresolved questions, Ethics in Medicine, fame study ffr, Fracional flow reserve, tagged ACC AHA ESC FAME TRIAL NEJM, evidence based medicine, FAME 3 TRIAL, multivessel pci, nejm on November 5, 2021|
News: Series of clinical trials fail to clear the ongoing confusion in the business of cardiac revascularization.FAME 3 is the new addition.
Caution: A non-academic journal review
There is no secret, about this cold war happening in an incognito mode for territorial rights between cardiologists and cardiac surgeons in glamorous cardiac suits for the past two decades. Of course, we keep believing this is a friendly fight in the overall interest of CAD patients. The ultimate winner should be the patient, not anyone else. Will that happen? Will anyone will allow that to happen? I am not sure.
The FAME3 is a stunning large study from 50 centers FFR guided multivessel PCI, that failed to dethrone CABG (or at least it wanted to sit along with it) I am not a seasoned statistician but definitely can’t understand the logic behind the methodology* and the choice of words in the conclusion from a paper published from a renowned journal.

(*I can recall an article about Non-inferiority trial from Lancet (Ref 1) )
FAME 3 aftermaths: A dizzy Interpretation
Before accepting the fact that, FFR guided PCI wasn’t able to show its superiority or to unable to prove its non-Inferiority, while CABG was clearly found to be non-inferior, (rather superior) to PCI, we should take into account an important caveat in the concept of FFR itself, which has at least half a dozen serious hyperemic and non-hyperemic flaws that demanded a more superior,non-hyperemic indices like iFR, RFR, qFR, etc.
Those of you who still believe PCI would be an undisputed modality in multivessel CAD should take up the challenge and disprove the superiority of CABG by doing the same FAME 3 subset with iFR and other stuff. (Eagerly waiting for the hypothetical iFAME 4 trial)
One more way to Interpret FAME 3: How can we accept FFR guided multivessel PCI as inferior, unless we have an FFR guided CABG (FAME 3 didn’t do this) to compare? Can you guess if only pre-CABG FFR was mandatory criteria, that would have excluded or included important grafts, what would have been the impact of CABG? This is a more dramatic suggestion, that will say sorry to FFR,( the old physiological friend,) and label it as a new villain.
Final message
Multivessel PCI still has a long way to go before trying to dethrone CABG. But, strictly scientific cardiologists need not worry much and they can continue to indulge multivessel PCI without FFR, which is no longer unscientific ! Thanks to FAME 3. I think one of the Important indirect consequences (?purpose) of FAME 3 would be, playing the end game for FFR.
Reference

“Unconquered” enemy of scientific research in medicine
Posted in bio ethics, Ethics in Medicine, evidence based cardiology, Medcal research, Medical education, Medical ethics, medical quotes, medical satistics, Two line sermons in cardiology, tagged evidence based falsehoods, evidence based lies, evidence based medicine, evidence based nonsense, experience based truths, principles of medicine on October 3, 2021|
Is there a solution?
As I understand, we don’t have any. Maybe, we can try this. No way, I can prevent it from appearing ridiculous for the mainstream scientists.
Truths often lie silently buried deep (many times intentionally). They definitely deserve an intellectual resuscitation beyond the dirty world of data and evidence. Further, why should experience be considered as enemy of evidence ?
Which is most important component in any medical research paper ?
Posted in Ethics in Medicine, evidence based cardiology, Medcal research, tagged duplicate medical research, ebm, evidence based medicine, finger criteria, how to do medical research, how to right a scientific paper, junk research, medical education, medical research ethics, rct randomised control trial, research methodology, student t test on September 11, 2021|
There are about 30000 scientific journals and two million papers every year. Of which 5000 are in medicine (Ref : World university news)
Now, take a deep breath and answer this query. What do you think is the most important aspect of any scientific or medical research in the current era ?
Final message
With due respect to all researchers, What do you think is the most important aspect of any scientific or medical research? This query is very much relevant today. All components are equally important is an easy way out. But, that’s not the pathway that will take us to the truth.
Postamble
Having answered the above question, no way, we can escape from this question –“Which could be the least important component “?
I guess you got it right. In the current scenario, my choice is striking and is sandwiched in the middle of the 7 responses..
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- August 2026 (1)
- July 2026 (6)
- June 2026 (9)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,713,332 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

