How can we use AI as a tool of knowledge distillation ?
Here is a deep discussion with Grok 3, on the merits, limitations & validity of DANAMI 2 and PRAGUE 2 , the two old studies on pPCI. Curiously , we don’t have any other studies to quote. As on 2025 , superiority of pPCI hangs precariously on these two decade old studies, which has some serious omissions in the primary end point and its Interpretation. To get into the facts , please go through the following link.
The therapeutics of coronary stenosis has become a technogical wonder, interwoven with statistical wordplay in the last few decades. PCI is sitting pretty at its peak glory.The term OMT or GDMT is a popular terminology, but realistically exist only in guidelines.
It is a strange academic habit among cardiologists, that they have subdivided medical management into optimal and suboptimal. Meanwhile, we haven’t seen any papers from cardiology forums that classify PCI according to its quality. How many of use a term like optimal PCI or guideline-directed PCI (O-PCI, GDPCI). Every PCI, by default, is perceived as good by our flawed coronary intellect.
A single patient experience
Let me share a patient consult from a remote town of north India. He is a STEMI patient (1 year old) with mild LV dysfunction and thinning of IVS and anterior wall. His CAG showed a significant looking, yet non-flow limiting LAD lesion without any troubling symptoms. I came to know he had consulted two institutions and was apparently not happy with their approach (In his own words, “They seem to be primarily interested in caging my LAD than listening to me”).
Somebody has suggested my name. He called me over the phone for a consult. I asked him remain there to follow his doctor’s advice. But, he flew some 2000 km to meet me. He was so knowledgeable and was aware of everything I wanted to tell. Like, viability, scars, futility, and benefits of revascularization, imaging-assisted PCI, impact of PCI on exercise capacity, importance of risk factor management, etc.
I told him, “In my opinion, you have technically a single vessel disease that can be managed well with drugs. But if PCI is to be done, it should be done in a proficient manner, as the lesion looked hard and was close to the LAD ostium, trespassing LCX as well.” I stressed the importance of a professionally done procedure with enough expertise and follow-up maintenance care.
He was not entirely satisfied with my response. He wanted a clear yes or no! . I told him, “If you have full trust, continue with the drugs at full intensity and do a stress test after 3 months. otherwise, if you keep getting even the slightest doubt and anxiety over the hidden blocks, go for a stent immediately at a good Institution. (My conscience said the latter half of my advice was unwarranted, but I had to; after all, me too need a protective mechanism)
He left my clinic profusley thanking me. I am not sure , how my consult was useful for him and what he is going to decide.
Academic lessons from this patient.
1.Patient fear factor over coronary blocks may be the ultimate game changer. Cardiologists should try to mitigate this fear and at the least should not be an amplifier to this emotion.
2.Leaving tricky profesionaly complex decisions to the patient, is an easy escape route for us, however it comes very close to professional incompetence. (Of course, we do this on a routine basis, approved by the modern medical guidelines, ethics, and legal system, in the name of patient empowerment)
3.Finally, we can grow a potential research hypothesis. A sub-optimal PCI is non-superior to OMT.It is curious there is no study available to compare sub-optimal PCI to OMT. We must also realize there is nothing called standalone PCI. Without concomitant OMT, PCI is a dud. Every young cardiology fellow need to etch this fact in their cortical cardiac memory. OMT often turns out to be the savior of stents, but the latter ruthlessly steals the credit.
Postamble
I could find one study analyzing suboptimal stenting (Ref 1), but it didn’t compare it with OMT. Suddenly, as I finish writing this, a big fact struck me hard, i.e., even a well-done PCI in sophisticated core labs with meticulous care struggled to beat OMT in a barrage of landmark trials (like COURAGE, ISCHEMIA, ORBITA). What is the big deal to analyze suboptimal PCI vs OMT?
A cath lab is an “optional accessory” in the management of Acute coronary syndrome (ACS).
True or False ?
Answer
“Without a CCU…you can never, treat any Acute coronary syndrome … while we can treat most ACSssuccessfully without a cath lab “ (If you still got the answer wrong …sorry, no comments)
Best comment
Accessory is ok , but it is “20% foolish” to state cath-lab is optional, it should be mandatory.
Bifurcation PCI is a modern-day Cardiologist’s fascinating professional adventure within coronary arteries. Of course, one of their Intentions is to do good for the patient. Bifurcation lesions (BFL) are a special subset of lesions, that looks challenging, more because of the potential biological aftermath following the delicate construction of a grade separator at a critical site. Mind you, it’s done within a live flowing artery and subsequently needs lifelong maintenance.
Strategies for BFL
Strictly committed* single stent strategy (Irrespective of what may come, LCX or LAD pinching let me take care . Don’t worry strategy *May sound dangerous, but still, it doesn’t make other strategies less ominous)
Provisional single stent strategy with elective cross-over for truly poor result /cosmetic/peer satisfaction purpose
Provisional single stent with bail-out cross-over. Often happen as an emergency (Not all techniques are amenable for this)
Elective planned two stents (Still, flexible to revert to single stent if the situation allows)
Elective, strictly committed, prefixed two-stent strategy (No going back strategy/ Not really a professional PCI )
Always remember, SYNTAX or no SYNTAX CABG is the safe & best bet for many severely symptomatic patients, with complex as well as non-complex BFL lesions esp in diabetic patients.
Wait, there are two more.
7. Please note, there is one benign strategy, that is always available, but hiding deep in the interventional cardiologist’s sub(non)conscious minds. It is a zero radiation, zero contrast, and almost zero cost strategy. Yes, It is “No stent strategy’ also called exclusive medical management, currently referred to as OMT/GDMT. In our analysis of symptom- lesions significance at least 30% of BFL are eligible for exclusive medical management.(FFR & IFRs ? Less we say about it, is better!)
8. One more option for those patients (&cardiologists) who wants to travel the middle path is POBA or a Glorified POBA ie DEB (Ref Corballis NH,. PLoS One. 2021)
Whatever the treatment, bifurcation PCI cannot be taken lightly. One exclusive club is debating this topic in Europe every year (EBC)for the past 10 years. Currently, Double kiss and crush (DK crush) is considered superior to others. Mini crush and Culotte are good alternatives in specific circumstances (Definition 2, NORDIC, BBC 2)
In DK crush every step appears to be double. Apart from the double stent, it is a double wire cross, double crush, double kiss, and double POT (or even more). All must happen in a specific sequence. One may add double Imaging (Pre and Post PCI IVUS or OCT) to the list. Finally and funnily not to miss the realistic possibility of double complications over the provisional strategy.
I am not sure which of the 10 steps in DK crush is most important. When we go through the physics of BFL intervention it appears, that proper crushing and kissing may be the key to success. Though kissing is an integral part of any two stent strategies, in DK crush it happens in a unique interface between balloons /balloons with a stent and finally between two stents. In fact
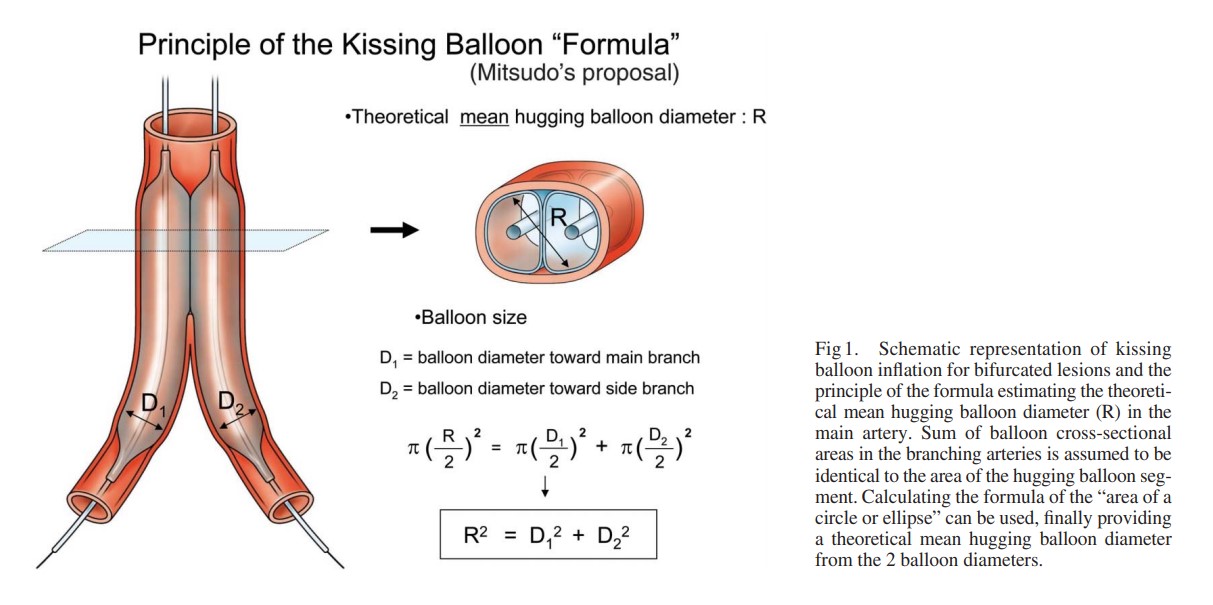
The physics of bifurcation kissing includes balloon hugging diameter, area, and pressure. Added to that is the intervening metal layer.
Can’t take the kissing in a casual manner. The Morino & Mitsuda model tells us more about the physics of kissing. In BFL interventions, kissing can happen with various layers that include one layer of the balloon with a crushed and non-crushed stent, carina. While we are mastering the techniques, we must realize, Kissing is aimed at stabilizing the carinal basement, still, there is a distinct possibility, that what may appear as innocuous kissing may undo all the good work we have done in previous steps. I guess, no harm in missing the final kissing if everything is ok in OCT.
Dr. Anonio Colombo’s take on kissing
Final message
So, we have both simple and complex modalities for BFL. Evidence and experience reveal that 90 -95 % of patients with BFL would be eligible for the easy path. In one sense, we are indeed wasting our energy and resources in tackling this negligible CAD burden located at the summit of the global CAD pyramid with a gigantic base. However, we can feel scientifically happy, that we have gained considerable expertise in tackling complex lesions with multiple stent strategies in recent times. Still, we are far away from a true vision, of what really might follow such a niche & expertise-intensive procedure.
Let us hope, that modern metallurgy in combination with physics & hydrology would ultimately beat Biology.
Looking at the whole issue of complex PCI philosophically, no technique may really be superior based on accrued evidence. In fact, when expertise becomes the key determinant, the evidence goes to the background. It is really surprising we are too much dependent on hasty and often biased evidence to ratify our expertise, technique, or hardware. I know, one of my colleagues can cross any lesion with one or 2 wires.
To insist, that a particular technique must be followed may not be academically correct always. It is similar to telling a coach driver in advance when to apply a brake or accelerator when he is negotiating multiple hairpin bends in hilly terrain on a rainy day, based on clinical trials done with different drivers on different routes. Ultimately, the outcome is decided by the expertise of the driver, the condition of the vehicle, the road, and not least, the destiny of the passenger.
This paper is to be presented in the the Forth coming Annual CSI meet New Delhi December 2012
Beware of Primary PCI : Is there a Low risk STEMI where pPCI is potentially contraindicated ?
Venkatesan Sangareddi . Department of cardiology . Madras Medical college
Primary PCI has proven to be the best option for management of STEMI . But it need to be done early, by an experienced team , in a good facility . It is not the individual expertise that matters ! Any treatment , which has great therapeutic potential also carries a hazard . So , these treatments must be used with caution. Not every STEMI patient , carry a high risk for death. In fact , the mortality in some of the subsets of STEMI can be as low as 1%. If , a STEMI patient , with a likely 1% mortality is going to get a procedure with 3 – 4 % ,risk it should (And Must !) raise a validity question But,this issue is rarely addressed in the interventional summits.
In a case pool of 56 randomly collected primary PCIs from various institutes , the outcome of pPCI was analysed .It is a retrospective , observational study .STEMI was graded as high risk when one of the following features were present and it was “low risk” when none of the feature was present ( Second STEMI , Extensive anterior MI , Class 3 /4 killip, An episode of VT/VF, Complete heart block, Diabetic individuals ) High risk STEMI constituted 22 patients .The overall in hospital mortality was (5/56) 9 % In high risk STEMI it was (2/22 )9.5 % in low risk STEMI it was 3/34 6.4 % .In the corresponding period 40 patients with STEMI who were treated by only thrombolysis or heparin (If beyond time window ) was used a control . 15 patients were in high risk In the this group the mortality in high risk STEMI was (3/15 )19% and low risk STEMI there was nil mortality (0/25) 0% .
There was an unacceptable moratlity with pPCI in the low risk STEMI which fared worse than even simple administration of heparin.These data reveal a dangerous fact , that is , primary PCI does not differentiate in the procedural risk with reference to the patient profile it deals with .While , it dramatically reduce the risk in high risk STEMI It confers a astonishing risk to low risk STEMI .The exact cause for this risk is not known . Common sense would tell , pPCI is expertise driven driven while thrombolysis is not .Our analysis also suggest bulk of early hazard of pPCI is also logistics related.
Primary PCI could be cautiously and consciously avoided in patients with low risk STEMI even if it is technically and academically indicated. This can have a great impact in the overall outcome of STEMI management.It is suggested every STEMI patient need to be risk stratified on arrival.(It is still a mystery , why we do this for NSTEMI and not in STEMI ) . A change in the current PCI guidelines to this effect is to be considered.
We do come across , even senior cardiologists , who tend to undermine the importance of poster presentations in scientific conferences (I know a few , who ridicule it as well ? ) .
Is it not a meanly job for a cardiologist to paste a poster and stand beside it for hours , waiting for scientifically motivated audience !
But , what really matter is the thoughts , concepts and often the hard work that brings these posters to big league conferences .
Please remember abstract posters must cross the hurdle of the conference peer review committee’s scrutiny . Often times the poster arenas has launched some crazy ideas , transform them to great discoveries.
If only , Gruentzig had shied away from the poster he famously pasted on lawns of ACC , Annual scientific sessions ,Florida
1975 . . . the revolutionary concept of PTCA would still be in utero !
Final message
I argue the young fellows in cardiology to send as many scientific abstracts as possible in their national or international meets . This is where the the future of cardiology lies ! Simply don’t bother about the critics .
Medical science has grown ( and growing ) in an astonishing pace. Many of the inventions which were considered as major break throughs have fallen on the wayside over the years . Of course , quite a few withstood the test of time .
One of the great inventions of last century is per-cutaneous interventions inside the human coronary artery .
The concept was first conceived and executed by Andreas Gruentzig of Germany in year 1977. Now , at-least a million PCIs are done every year to tackle CAD with greatly improved knowledge base, evidence , hardware, techniques and expertise .
PTCA is an invention worth a Nobel prize . . .well , that’s what we cardiologists feel. The Nobel committee seems to think otherwise .
What could be the reasons ?
PTCA is simply an extension of an old invention. Already the inventors of the cadiac catheterization were conferred with Nobel prize (Forssman, Cournand,Richards) . Hence , it is a sort of duplication of invention . If Gruentzig is conferred a Nobel prize the man who discovered the coronary stent (A plaque scaffolding device) will argue he too deserve a Nobel !
What Gruentzig did was in-fact a fundamental human response by Instinct ! .When you encounter a mechanical obstruction on the road just try to overcome it . “Here is an obstruction impeding the blood flow , let me remove it” . He did this with a wire and balloon . There is not much intellectual innovation . It was delivery of a mechanical force through a wire . But what the Nobel committee should take it to account is , he did this in live human beating heart and cured of his illness most dramatically avoiding a need for surgery.
Finally comes the vital question. What is the impact of this invention in the health of mankind. ? How many lives have been saved when compared to other modalities to treat the coronary artery disease ? *.This again is not convincingly answered especially in stable angina , for which Geuentzig originally developed this modality . One popular argument is , in terms of life saved and sufferings relived oral rehydration fluid or penicillin would beat PTCA most convincingly !
* Another possible reason is , the Nobel medical committee is probably well aware of the perennial controversy about role of Medicine vs Surgery vs PCI on the outcome CAD and the superiority of one over the other !
Final message
Whatever be the reasoning , Nobel committee has to rethink . Cardiologists all over the world would definitely agree if one man who have made a huge difference in their patient’s life , it must be Gruentzig .
It is well-known Nobel prize is given for path breaking research that break new grounds like decoding cosmic mysteries , expansion of universe , cell signalling , molecular mimicry and the stuff like that .
Still , Gruentzig definitely deserves a Nobel solely for the novelty in his procedure and in the process it helped avoid surgery in vast majority of heart patients.
This term is quiet often used in the main stream cardiology journals , in work places , conferences , hospitals and even among lay persons . No body bothers to define this terminology. What exactly this term means ?
It may not mean anything . . . to most of us even as the percentage of inappropriate angioplasty is steadily increasing over the years .
Picture courtesey : Jupeter Images
What does the term Inappropriate angioplasty mean ?
(Choose the correct answer . . . one or more may be true )
A.It simply means doing unnecessary angioplasties and has no major implication to any one.
B.A form of medical ignorance or an unethical act and should be strongly condemned.
C. An acceptable cardiology practice , need not be discouraged , as it improves the quality of life of physicians !
D. A sure act of “error by commission” that amounts to medical negligence .
E.It is a decent term for a major guideline violation
E. It can be termed as medical malpractice as it amounts to harming the patient with or without intention.
When PTCA was introduced by Gruntzig in 1977 the whole world was awestruck. All he did was . . . to dilate a coronary stenosis with a balloon. No scaffolding was ever thought off at that time. It was a huge achievement . PCI version 1 was performed for over 20 years in nearly a million patients . Till his death stenting was an unknown concept.
When the stents first came in, it was first used with extreme caution . From the days of bail out stenting, it has evolved into provisional stenting, elective stenting ,and now what is called “mandatory stenting”
When Greuentzig was able to perfuse the obstructed coronary arteries successfully in thousands of patients in the 1980s, with a simple balloon
. . . what is the difficulty for us to replicate it in 2011 ?
Unfortunately advocates of POBA (Plain old balloon angioplasty) are considered to be un-scientiifc cardiologists or even carry a risk of labeled as quacks.
But please remember . . . POBA is alive and doing well too , in spite of the serious threat it faces from the current generation interventionists . It will continue to have an important role in many situations.
1.In patients with multivessel disease while the proximal lesion deserve a stent , POBA is preferred in distal lesions to reduce the overall metal load .
2.POBA has a major role to play in Primary PCI .We need to realise dying myocardium does not demand for stents. It simply requires quick and prompt restoration of blood flow. POBA can achieve this with flying colors in most situations.
3. Further , stenting may be difficult in complex lesions during primary PCI .Experience tells us , it is dangerous to prolong the primary PCI procedure time. Here POBA is the only choice , may be assisted by thrombus aspiration. Stenting may be delayed or even avoided in many STEMI patients. . We know there is huge STEMI population with pure thrombus with no atherosclerosis.
4.Patients with co morbid conditions , who are likely to have a non cardiac surgery in the near future and those who can not take antiplatelet drugs POBA will score over BMS/DES.
5.Finally a POBA costs nothing . .All it requires is a stiff balloon . In this recession prone world and ever increasing incidence of CAD , POBA could be the answer.
6. Acute recoil in POBA (Sudden deaths in POBA is a rare event !) are more of a perceived fear rather than a reality. It can be argued stents are primarily used to make cardiologists job easy and comfortable.
7.Cost effectiveness of plain balloon verses stenting was never properly tested .
Final message
When sudden deaths due to subacute thrombois in DES population is accepted with all those attendant pride . . . why not we accept a risk of less sinister event namely the late onset restenosis with POBA.
This is a funny world . The DES fiasco is driving us towards stent less world and a bio degradable stent is already being projected as new savior.
Meanwhile no one can kill POBA thats for sure ! It will ultimately be reinvented with another exotic study soon !
Reporting a coronary angiogram may look like child’s play for most cardiologists. Many do it in less than a minute. (It goes something like this 90 % LAD , 30 % ostial OM1, 50 % mid RCA etc etc ) The famous and meticulous classification of Ellis and Ambrose proposed two decades ago appear largely redundant.
In this review we shall briefly debate an eccentric plaque or lesion .
Pathological definition
Pathologically an eccentric lesion will have a disease free arc within an atherosclerotic lesion.If we apply this criteria most of the plaques appear to be eccentric.
Angiographic definition
In simple terms eccentricity is said to be present when the plaque volume is three times more on one side when compared to opposite side .
The incidence of eccentric lesion is largely under estimated. It can be up to 40 % of all lesions.
It has histological as well as hemodynamic significance.
How to measure eccentricity index ?
Ratio between maximum plaque thickness and minimum plaque thickness (Including the media )
Image courtesy modified from Circulation. 1996;93:924-931
In the above figure : The eccentricity index is measured as the ratio of the maximum to minimum plaque plus media thicknesses. In the eccentric lesion the maximum wall thickness measures 2.6 mm, minimum wall thickness measures 0.2 mm, and eccentricity index is calculated to be 5.2. In the concentric lesion the maximum wall thickness measures 2.2 mm, minimum wall thickness measures 1.6 mm, and eccentricity index is calculated to be 1.4.
What are the associations of eccentric plaque ?
Calcification and hard plaques are more common in eccentrically placed plaques.The most vulnerable point for plaque rupture or disruption is the shoulder region between normal and plaque segment.
A long eccentric lesion with over hanging plaque
Clinical implications
Acute recoil
Coronary spasm
Mechanical effects : Asymmetric expansion of stent
Drug eluting stents
An arc of normal plaque circumference predispose to acute recoil and spasm.this is logical as the normal arc will have a fully functional medial smooth muscle which are prone for spasm.
Does stenting reverse the eccentricity of plaque ?
It may not . The drag effect of major plaque mass may either result in plaque prolapse or asymmetric stent approximation or even stent crushing effect.
How does the the stents elute in an eccentric lesion ?
Stents are not intelligent enough to differentiate the plaque surface and normal surface. We also know these drugs are toxic to normal endothelium and hence are not welcome in the normal arcs of an eccentric lesion.
Since the drug secretion is uniform throughout the circumference it makes the DES a perfect misfit in eccentric lesions As we realise most of the lesions are pathologically eccentric one can guess the long term consequences .
Final message
The more we think we know . . . the less is understood .
The images we see daily in cath labs are too simplistic to make vital decisions .There are constant innovations coming up but none seems succeed in imparting common sense to majority us.(Namely direct plaque intervention can never succeed over a diffuse medical disease called atherosclerosis )
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.